Summary box
Conchal cartilage is adequate for the majority of nasal reconstruction.
The morbidity of graft harvest is not trivial.
Care must be taken during harvest, especially in elderly patients, to avoid breaking often brittle cartilage.
Great care must be taken during cartilage inset to ensure complete soft-tissue apposition to the cartilage graft
Banked costal cartilage provides excellent quality and volume of cartilage for grafting without donor-site morbidity.
7.1 General Considerations
The use of cartilage grafting in nasal reconstruction is liberal and is used to both replace resected cartilage and reinforce areas that anatomically lack cartilage but will require support to prevent deformity in healing. This is most applicable in partial or total alar reconstruction where both anatomic and nonanatomic cartilage grafting can prevent irreversible alar retraction and deformity. 1
The requirements for a successful cartilage graft include a robust vascular bed and firm suture fixation to support its ingrowth and prevent extrusion and subsequent infection.
The selection of donor site for cartilage grafts is based on the needed graft size and shape, consideration of the donor-site surgical access and postoperative morbidity, as well as the shape and size of the cartilage. The majority of isolated lower third nasal defects can be managed with conchal cartilage grafting or MTF cartilage. Defects larger than isolated heminasal will require rib cartilage grafting or multiple MTF cartilage grafting.
7.2 Donor-Site Selection
7.2.1 Conchal Bowl Donor Site
The conchal bowl is an excellent donor site and provides robust flexible cartilage that, if harvested contralateral to the defect, approximates the shape of the native alar cartilage. Provided the antihelical fold is not violated, the entire cymba and cavum conchae can be harvested with minimal donor-site morbidity and no change in the final appearance of the ear. 2 Preoperatively, the patient should be asked about any hearing aid requirements, given this requirement can be a contraindication. For patients who do require hearing aids, the conchal bowl donor site is not suitable, given the long-term pain and difficulty in fitting the expensive prosthetic hearing devices. When the side that the patient prefers to sleep on has been determined, then the contralateral side is chosen for harvest as long as the alar shape requirement is not required. During the surgical preparation, the external auditory meatus, as well as the front and back of the external ear, is carefully prepped. The patient is placed on a sterile towel and great attention is directed at maintaining sterility throughout the process, which includes avoiding contact of the patient’s hairnet or nonsterile head dressing with the ear.
Lidocaine mixed with epinephrine and 0.25% Marcaine is injected subcutaneously with a 27-gauge needle both anteriorly and posteriorly on the conchal bowl, and the local anesthetic injection is used to hydrodissect the skin from the cartilage. Either an anterior or posterior incision can be made. The advantages of an anterior incision rely on a significantly easier harvest, as well as an easier access to the incision for postoperative care with no sacrifice in donor-site scar appearance. The entire conchal bowl is sharply dissected with an assistant holding the dissected skin flap up out of position and then the entire conchal bowl is carefully managed with Adson-Brown forceps versus regular Adson forceps and then sharply dissected free of the donor site. At this point, careful hemostasis is achieved and then the donor site is simply closed with a running horizontal mattress, 5–0 plain gut suture taking care to ensure eversion approximation of the wound edges. No external bolster dressing is required; however, the dead space must be obliterated to prevent formation of late hematoma, and multiple through-and-through 4–0 gut sutures are placed from the front to the back of the ear with a straight Keith needle and the suture is tied on the anterior aspect of the ear. The ear is liberally coated with antibiotic ointment and followed carefully during the postoperative period to ensure healing without hematoma or infection. No postoperative antibiotic coverage is provided; however, if the patient does develop a postoperative infection at the donor site, wound cultures must be taken and prescribed antibiotics must include pseudomonas coverage, given this can be a frequent pathogen. 3 In elderly patients, the gradual increasing in stiffness of the cartilage must be considered and significant care taken in the graft harvest, given that it is increasingly brittle and prone to fracture.
The cartilage is harvested with perichondrium intact on both sides and carefully thinned and contoured and sewn in place with 4–0 Vicryl sutures to a carefully designed and approximated cartilage pocket. Even small toothpick-sized segments of conchal cartilage can be utilized and these can prevent late alar retraction if placed in a properly designed subcutaneous pocket in a nonanatomic location along the alar rim.
The difficulty in harvesting conchal cartilage grafts lies only in harvesting adequate length and this must be ensured prior to incision and rarely is the vertical height or width of the graft a limiting factor (▶ Fig. 7.1, ▶ Fig. 7.2, ▶ Fig. 7.3, ▶ Fig. 7.4, ▶ Fig. 7.5, ▶ Fig. 7.6).
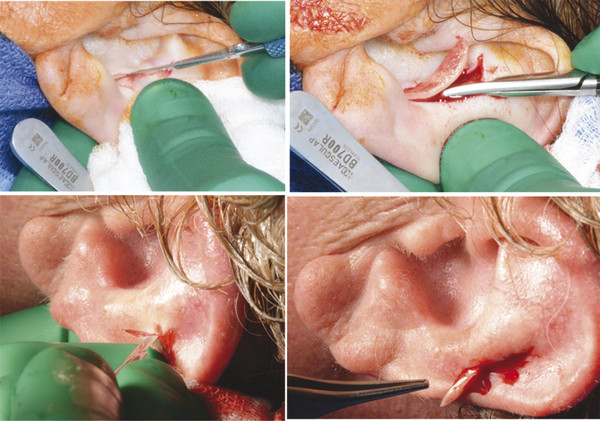
Fig. 7.1 Although conchal cartilage harvested form an anterior approach to the entire conchal bowl constitutes the majority of grafts, the anterior helical rim is also a suitable donor site. If more cartilage is required, the entire conchal bowl may be harvested.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


