A youthful periorbita is essential in facial rejuvenation. Injecting the periorbital region requires a deep understanding of anatomy, filler characteristics, possible complications, and treatment goals. The tear trough deformity is characterized by a sunken appearance of the lower lid that may yield a dark shadow resulting in a tired appearance. An esthetic lower eyelid should have a smooth transition to the cheek/malar subunit with no obvious discoloration. The article will present important understanding of anatomy, possible complications, and management, and will compare needle or cannula to achieve safer, reliable results. Finally, the senior author’s personal technique using both needle and cannula injection will be described.
Key points
- •
Always perform a full facial examination and assess the need to treat adjacent subunits first.
- •
Ensure appropriate knowledge of possible complications and their management prior to injecting in this region.
- •
The pre-periosteal plane is the preferred method of administration with small aliquots and close follow-up.
- •
Neither cannula nor needle demonstrated superiority in clinical trials.
Video content accompanies this article at http://www.advancesincosmeticsurgery.com
Introduction
“The eyes have one language everywhere.” – George Herbert
A youthful periorbita is essential in facial rejuvenation. Injecting the periorbital region requires a deep understanding of anatomy, filler characteristics, possible complications, and treatment goals. The eyes have long been described as the center of the face and with the increasing demand for non-invasive or non-surgical treatments for periorbital aging, many novice injectors are starting to venture into this region with little understanding of the possible complications and adverse outcomes that may occur. The periorbital region is home to the thinnest skin in the body, with multiple complicated ligamentous, arteriovenous, muscular, and fat structures [ ]. To further the confusion, there is widespread debate and discussion regarding the use of a cannula versus a needle in periorbital injections, especially in the lower eyelid and tear trough. The tear trough deformity is characterized by a sunken appearance of the lower lid that may yield a dark shadow resulting in a tired appearance [ ]. An esthetic lower eyelid should have a smooth transition to the cheek/malar subunit with no obvious discoloration.
There are a whole host of different classification and grading scales that have been published describing different methods of characterizing and assessing the infraorbital deformity [ ]. Without consensus, however, these may further add confusion and complexity to the already elusive problem at hand. As will be described further in the article, it is the author’s opinion that a more comprehensive evaluation, such as the Facial Assessment Scale (FAS) by Galderma (Lausanne, Switzerland) provides injectors with a better idea of treatment goals, and specific attention must be placed on adjacent subunits to improve the whole region [ ].
This article will focus primarily on the lower periorbital region, given that it is more commonly addressed. The article will present an important understanding of anatomy, possible complications and management, and will compare needle or cannula to achieve safer, reliable results. Finally, the senior author’s technique will be described with a video.
Anatomy
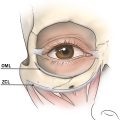
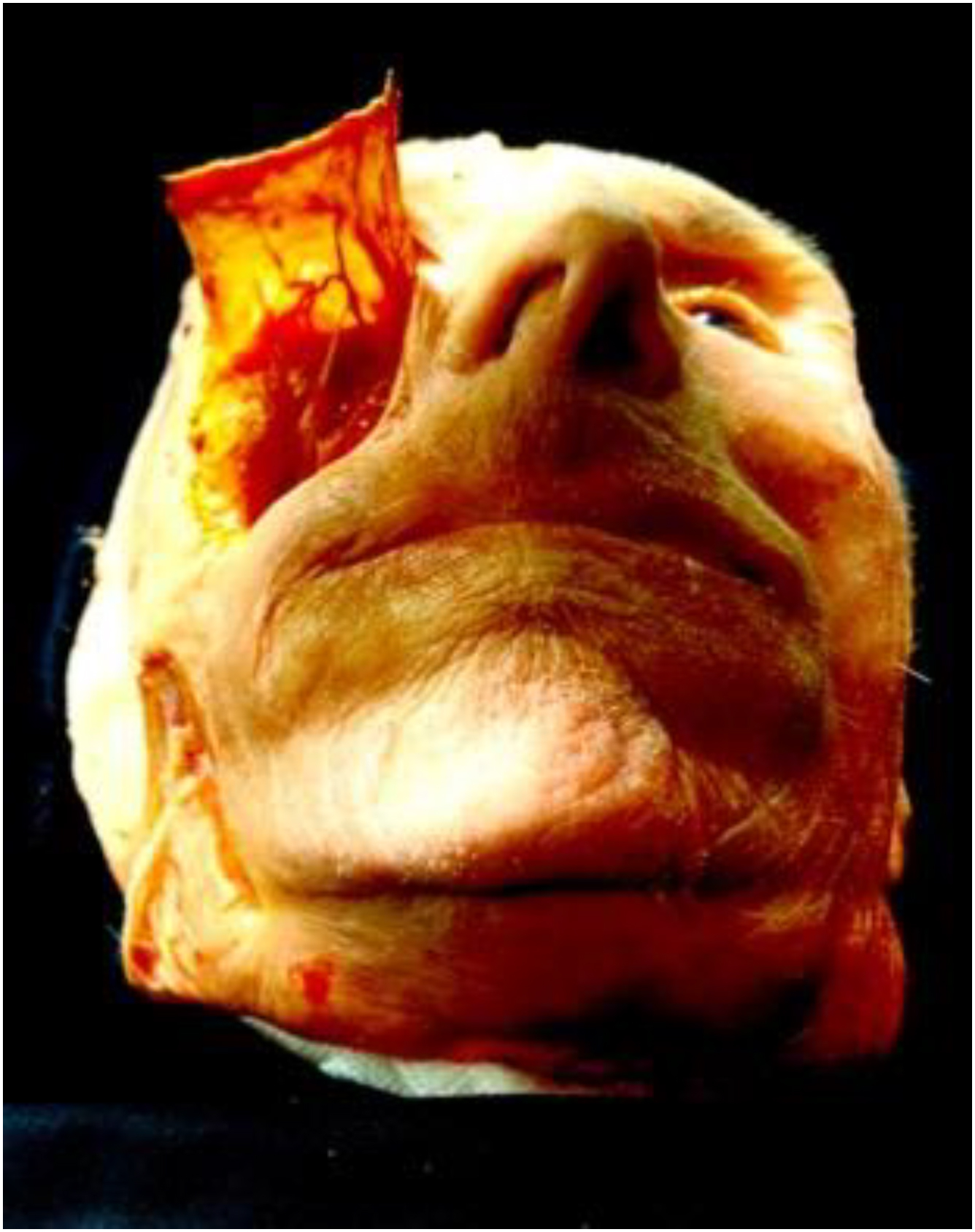
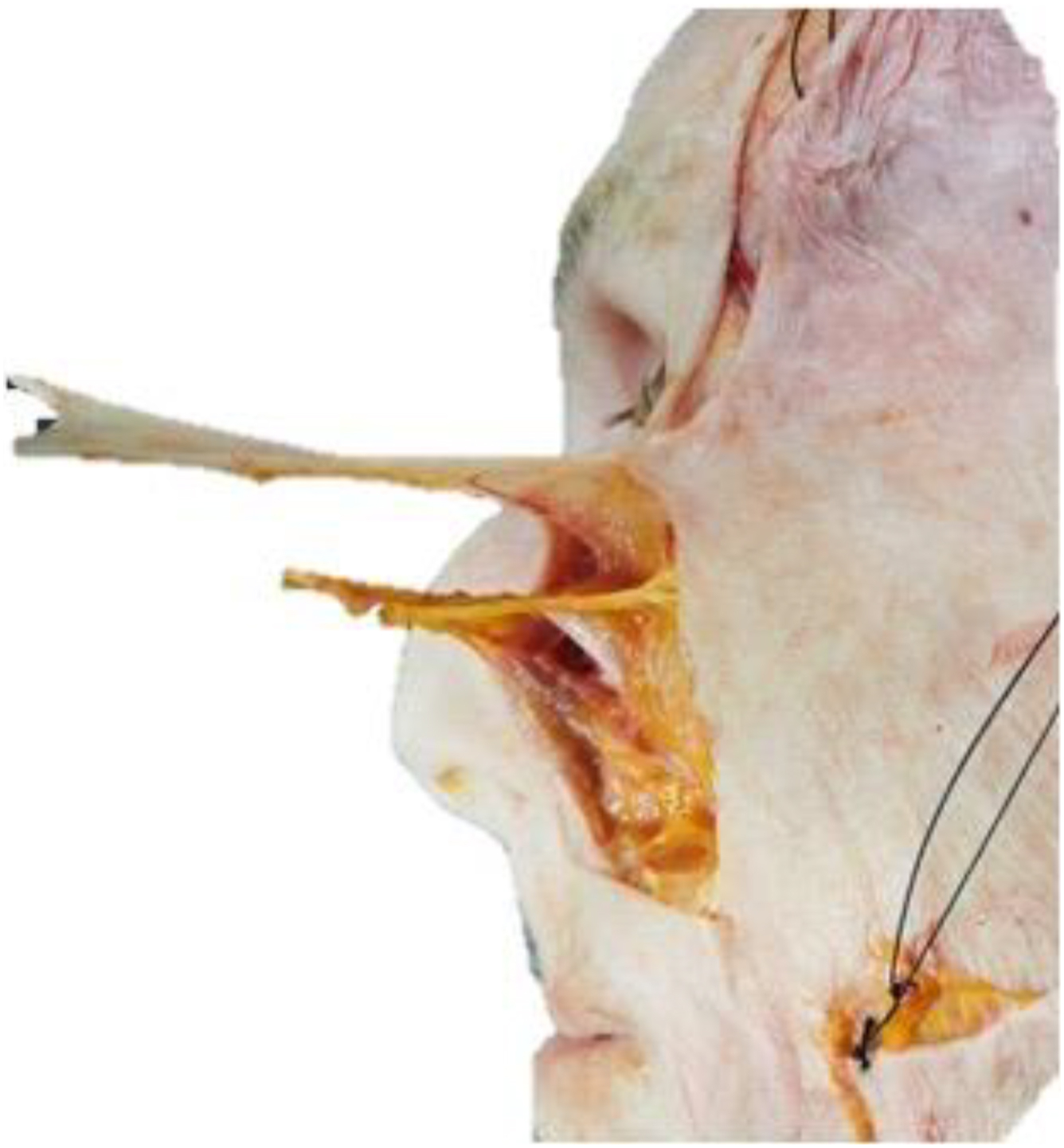
The anatomy of the lower eyelid is complex and is the primary reason why injectables in this region are prone to irregularities and adverse events (AEs). Firstly, the skin measures less than 1 mm with minimal subdermal fat [ , ] ( Fig. 1 ). The tear trough anatomic etiology has long been studied and discussed. There exists a true osteocutaneous ligament that continues to form a bilayered orbital retaining ligament which are arranged circumferentially around the orbit [ , ]. Medially, it is referred to as the tear trough ligament and has been shown to insert onto the bone adjacent to the medial canthal tendon. The orbicularis oculi muscle is divided into its orbital and palpebral components by this tendon and has been shown to be strictly adherent to the bone at the level of the tear trough ligament [ , ]. The zygomatic cutaneous ligament is found just above the origins of the levator labii superioris in the medial infraorbital region [ ] ( Fig. 2 ). Anatomic studies have demonstrated that it originates along the medial arch and lateral malar body. It then covers both the zygomaticus major and minor muscles and the levator labii superioris medially [ ]. Here, it rejoins the orbicularis retaining ligament (ORL) at the region of the tear trough ligament, with the confluence of the levator labii superioris and levator labii superioris alaeque nasi muscles [ ]. Sitting between the ORL and zygomaticocutaneous ligament in the preperiosteal plane is the sub-orbicularis oculi fat (SOOF). See ( Fig. 3 ) Additionally, at this region is where the formation of malar mounds or edema occurs. It is hypothesized that with the strict ligamentous attachments and limited lymphatic drainage, this is why there is an excess of edema/swelling post injection in this region [ ].

It is crucial to understand the arterial anatomy given the risk of embolization and blindness. The infraorbital artery exits the infraorbital foramen with the infraorbital nerve and is located medially one-third of the distance between the medial and lateral canthus. One study reports this distance on average to be 6.3 to 10.9 mm below the rim and does not change with aging [ ]. Laterally, the zygomaticofacial artery runs with its corresponding nerve through a foramen that can be 0.5 to 0.6 cm lateral to the orbital rim [ ]. It is not always present, having only been found in one-third of cadaver dissections. Most importantly, at the most medial extent is the termination of the angular artery which anastomoses to the dorsal nasal artery. It is superficial in position which significant variation, even coursing laterally in 30% of Asians. Given this anatomy, this is why the pre-periosteal plane may be considered the preferred location for placement of product [ , ]. Lastly, 1 important structure is the angular vein which is found in the most medial aspect of the tear trough and can also contribute to some of the blueish hue seen in the infraorbital hollow [ ].
Lastly, aging has its effect on all layers of the periorbita. Well studied phenomena have demonstrated that the maxilla undergoes clockwise retrusion from the lateral view, causing descent and ptosis of the overlying soft tissues [ ]. This soft tissue descent coupled with increasing laxity of the retaining ligaments, and orbital fat herniation leads to a worsened infraorbital hollow.
Cannula versus needle
It is important to first understand what the reasons are one would favor the cannula to the needle. The needle provides a sharp point to be able to theoretically place the tip where the product needs to be. It can traverse planes without issue but cause trauma as the tip passes through tissues. This can cause bleeding, bruising, or further discomfort. The cannula is proposed to be less traumatic to the tissues, therefore causing less bruising and bleeding. However, it still requires an entry point and can be difficult to navigate through planes in a precise fashion, especially when using a larger gauge.
One systemic review comparing needle to cannula injection, mentioned that hypodermic cannulas should reduce the risk of inadvertent arterial or venous cannulation [ ]. Theoretic studies have demonstrated this proposed decrease risk of inadvertent placement with a cannula. One cadaver study demonstrated that the use of a cannula was able to maintain the product in a given plane more readily than the use of a needle. However, there was an increased risk of backflow, which could still be dangerous should an arteriovenous structure be punctured through and through on entry [ ]. One comment by the authors was that the use of needle actually resulted in the product moving more superficial. These findings were then confirmed with another cadaver study that demonstrated similar findings, that the filler placed with a needle was more likely to transverse more anatomic planes as opposed to the cannula-based injection with a 25 G cannula. In this study before disclosing the findings, participants were surveyed and believed that needles were more precise, which was not the case. They do correctly identify that the tissue planes were likely much easier to traverse in the cadaver versus live patient and tissues. This may be 1 of the reasons the cannula technique was successful in reaching the preperiosteal plane in all cases. The systematic review also demonstrated that comparing needle to cannula injection in the lower lid found that patients tolerated the needle-based injection more; there were similar complications in both groups. In terms of technique utilized, there were many techniques employed with the needle group including deep scaffolding (1), fanning/layering (1), retrograde linear threading (2), push-ahead (1), deep fill (1). The cannula group utilized a majority of retrograde (4) or fanning (3). Needle size ranged from 27 to 32 gauge, with the 30-gauge needle being the most frequent (65%). Size range was larger among the cannula-based articles (18–30 gauge), with the 25G being the most frequent. Unfortunately, in conclusion, no one technique or technology can be deemed safer from this review.
Similar findings were published in another review of prospective trials by the senior author of this article [ ]. Sixteen articles were included; however, they found through a meta-regression analysis that subjects treated with needles had a statistically significant greater incidence rate of ecchymosis, compared to those treated with cannula. Conversely, subjects treated with cannula had a statistically significant greater incidence rate of edema, compared to those treated with needles.
The needle configuration, as demonstrated previously, traverses the tissues using the tip of the needle; however, when injected will come out the bevel side and possible flow in a retrograde fashion. The cannula, with the opening being just posterior to the blunt tip, necessitates a more parallel entry point to the direct needle placement. This inadvertent superficial placement of product has been hypothesized to be the cause of persistent malar edema after injection. It is important to ensure that the needle’s angle is respected, and the bevel is down onto the desired plane to reduce the risk of inadvertent superficial spread [ ]. One study, examining the use of needle-based injections in a perpendicular plane, found that on sonographic evaluation they were able to successfully fill the suborbicularis space with their 3-point injection technique [ ]. They used on average a total of 0.45 mL ± 0.14 mL. All patients were brought back at 1 week, given the need to undercorrect their tear troughs; however, 90% required a second top-off of injections. Regardless, perhaps the multiple injection points allow for less product to be placed in one particular area causing more retrograde flow or diffusion through planes.
One study of the only randomized controlled studies that has been performed utilized HA R (hyaluronic acid) (Restylane, Q-Med AB; Uppsala, Sweden) to correct the tear trough deformity [ ]. They randomized patients and compared either a 27G cannula or 29/30G needle. Interesting findings included that age did not correlate with an increased amount of product required, amount of product, and second visit numbers were not significantly different between the cannula or needle group. There was no significant difference between AEs, including edema, pain, and ecchymosis. One commentary identified that the 27G cannula may in fact behave more like a needle than a cannula, thereby still causing local trauma to tissues [ , ]. Additionally, the visibility of the filler may be due to undue placement, superficial placement, retrograde flow through the needle, or even through traumatic or senile changes to the orbicularis oculi muscle [ ].
Another multicenter, observational, single-blind study demonstrated that in a total of 1200 patients treated either with a 30G needle (35.7%) or 25G cannula (64.3%), no touch ups were required with the needle, but 18.4% of the population required with cannula injection [ ]. The authors also comment that small boluses using the cannula may lead to better overlying support and less visibility when compared to linear threading. They go on to specify that in their practice the use of a cannula leads to more superficial placement and overcorrection, given the tendency to go more superficially. Interestingly, when compared to the randomized control trial mentioned earlier, they used a larger gauge cannula that may be more difficult to navigate to the appropriate plane as with the 27G cannula.
Now treatment of the tear trough or infraorbital hollow has been primarily volume restoration with little focus on the tear trough ligament itself. In surgical correction, this ligament is ablated either through direct visualization and surgical disruption or through the use of a fat grafting cannula in a blunt fashion. In a similar fashion, 1 technique was designed to utilize a 25G cannula to stretch out the tear trough ligament insertion and then fill the void with HA. When compared to filling alone, patients received significantly less product with the novel stretching technique (0.3 cc [0.2cc–0.3 cc]) versus (0.6 cc [0.6cc–0.8 cc], P < .001). Additionally, patients without ligamentous stretching had higher rates of surface irregularities [ ].
In all, it seems that the present literature does not give us a clear and concise answer as to which technology will yield the best result. What does become clear is the product should be placed in multiple boluses and on the preperiosteal plane to help avoid any surface irregularities [ ] ( Figs. 4 and 5 ).