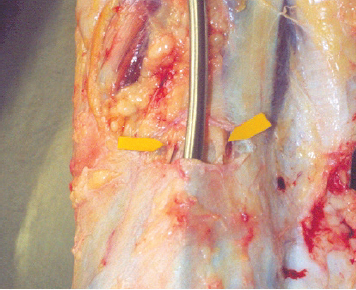
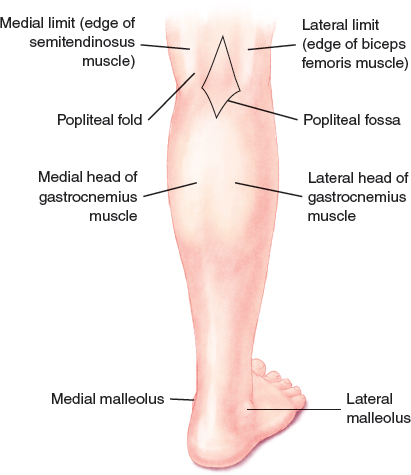
CHAPTER 19 Often the strong fascia of the calf prevents an increase in muscle mass, even among weight lifters. This leads to a lack of harmonious contour that can be corrected with an implant. Calf muscle atrophy resulting from congenital or acquired disease is not unusual; although polio has been nearly eradicated, it is still one of the primary causes of calf muscle atrophy. Calf implants are designed to enhance the volume of the calf by imitating the shape of the gastrocnemius muscle. In most patients, augmentation of the medial head of the muscle is sufficient to reshape the leg, and only one implant placed medially is used. For patients undergoing reconstruction, however, there are indications to use implants over the lateral head of the muscle to obtain the proper shape. The posterior aspect of the calf is not a good area for implant placement, because the small saphenous vein crosses this area, and the device can compromise blood flow. The variety of possible hypoplasia types and symptoms requires that a thorough examination of the patient occur before the selection of a specific treatment or implant. The implant size, type, and site should be reviewed with the patient during the first office visit. It is important to clearly understand the patient’s complaint before any decisions are made. Several silicone calf implants are on the market, and they can be divided into two types: gel-filled implants and elastomer implants. Both are excellent choices for most patients, and each type has distinct qualities, advantages, and disadvantages. Textured devices must be avoided, because they are most likely to produce a seroma. The two most important features of calf implants are their shape and size. Implants that are too large are a poor choice, because they can reach the posterior medial line of the leg, which is the location of the small saphenous vein. The appropriate implant size for most patients is 4 to 5 cm wide in the medial area and 14 to 19 cm long; the volume of this size implant is 140 cc. On the lateral aspect, the size used should be smaller than the medial. With calf implants, knowledge of the surface anatomy is particularly important, because the objective of the procedure is to reproduce the shape of the muscles and the features of the natural anatomic surface. The medial and posterior aspects of the calf have muscles and tendon projections that allow easy identification of most of the muscles. The “goosefoot” formation is composed of the joint insertion of the gracilis, semitendinosus, and semimembranosus tendons found at the medial posterior area of the knee, and the biceps femoris on the lateral surface limit the popliteal area. The gastrocnemius muscle and tendon are palpable and visible, as is the popliteal fold, which is formed by the leg flexing over the thigh at the popliteal area. Fig. 19-1 The gastrocnemius or calf muscle is formed by two large portions: the medial head (larger and longer) and the lateral head. It is the largest muscle of the leg, and it works as a powerful postural and locomotor muscle that flexes the foot and knee. The medial and lateral heads originate close to the medial and lateral condyles of the femur, respectively, and they insert like membranous sheets that fuse with the soleus tendon to form the calcaneal or Achilles tendon. The fascia of the leg is quite thick, especially in the anterior and caudal areas. It is composed of oblique and vertical fibers that intercross transversely to form a very strong mesh that passes in front of the tibia at the medial face and that is strongly inserted over the tibia to create a single structure with the periosteum. The leg fascia and its compartments make the muscles compact and potentiate their action while simultaneously creating a stable container that helps regulate the internal pressure, thereby helping the venous return system via the deep veins’ valves. The leg fascia connects to the thigh fascia at the top and to the foot fascia at the bottom without interruption. The contraction of the leg’s muscle mass compacted within the fascia helps drive the blood contained within the deep veins. Because this fibrous tube acts as an inelastic container, any increase in its contents can exert external pressure on the vessels in the area, thereby reducing the lumen and impairing blood flow; this is known as compartment syndrome. Fig. 19-2 The tubular structure formed by the fascia of the leg is divided internally by septa that create three tubular fibrous compartments: the anterior, lateral, and posterior compartments. Each compartment contains a group of muscles with similar actions and regular innervation. These compartments are formed by two septa that originate at the fascia and then vertically insert at the anterolateral and posterolateral edges of the fibula (the anterior and posterior muscular septa, respectively) and by the interosseous membrane that inserts into the tibia and fibula. Fig. 19-3 The posterior compartment is the largest compartment of the leg and contains eight muscles. There are really two compartments—the superficial compartment and the deep compartment—that contain four muscles each. The transverse septum between the muscles, also called the deep sural septum, divides the posterior compartment. All of the muscles in both the superficial and deep parts of the posterior compartment are innervated by the branches of the tibial nerve. The gastrocnemius (the medial and lateral heads) and soleus muscles are in the superficial part of the posterior compartment, which form the sural triceps; the small plantar muscle is found more deeply and medially. The calf implant will be placed in the superficial part of the posterior compartment. The great saphenous vein runs under the subcutaneous tissue and lies outside the fascia of both the leg and popliteal area. It is important not to go beyond the edge of the semitendinosus when a medial incision is made to avoid the great saphenous vein, which usually lies more toward the middle portion than the edge. Although the recommended incision does not affect this vein, it is important to know the vein’s location. In the previous photograph of a dissected cadaver, the great saphenous vein is visible 2 cm away from the edge of the semitendinosus tendon. The incision used to access the subfascial compartment was started at the medial edge of the semitendinosus. The same technique is done during the actual surgery to avoid damage to the great saphenous vein. Usually the small saphenous vein runs subcutaneously to the middle of the leg, where it goes deeper and perforates the fascia to join the popliteal vein. The level of penetration varies. In some patients the small saphenous vein joins the popliteal vein above the line of the posterior knee fold. If this is the case, the medial part of the incision, if elongated, could contact the vein in the subcutaneous tissue of the popliteal fossa. If the small saphenous vein penetrates the popliteal vein under the fold, it may be found by forcing the undermining close to the posterior part of the calf between the two heads of the gastrocnemius muscle. If lateral undermining must be performed to introduce a lateral implant, undermining at the posterior portion may be avoided if a lateral incision is made. The common fibular and lateral cutaneous sural nerves are especially prone to damage when a lateral incision is made. Only a digital undermining maneuver should be used under the fascia; scissors should not be used in the intrafascial space, and a minimal amount of traction should be used at the medial edge of the biceps muscle on the thigh to avoid damage to the common fibular nerve. After the fascia has been entered, this nerve is easily palpable and can be felt with a finger by pressing laterally near the biceps. The nerve resembles a thin tendon close to the muscle’s edge.
Calf Implants
Calf Implants: Their Indications and Placement
Surgical Anatomy
THE GASTROCNEMIUS MUSCLE
THE LEG FASCIA
THE TUBULAR FIBROUS COMPARTMENTS OF THE LEG
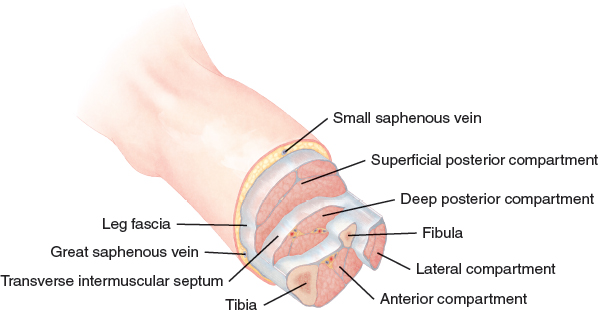
THE POSTERIOR COMPARTMENT OF THE LEG
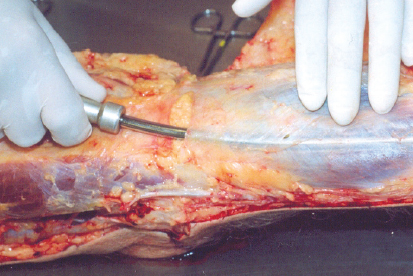
THE GREAT SAPHENOUS VEIN
THE SMALL SAPHENOUS VEIN
THE COMMON FIBULAR AND LATERAL CUTANEOUS SURAL NERVES
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine