Nakagawa T, Takaiwa T. J Dermatol 1993; 20: 558–60. The use of these agents in patients with renal insufficiency may result in aluminum toxicity.
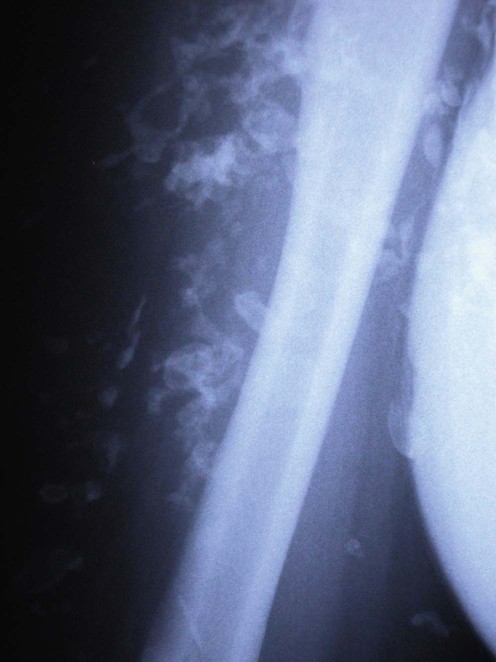
Calcinosis cutis
First-line therapies
Calcinosis cutis in juvenile dermatomyositis responsive to aluminum hydroxide treatment.
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

















 No treatment/self-healing
No treatment/self-healing Aluminum hydroxide
Aluminum hydroxide Intralesional corticosteroid
Intralesional corticosteroid Diltiazem
Diltiazem