Key Words
burn wound management, burn wound contracture prevention, burn wound infection, burn wound complications, wound debridement, pain management
Synopsis
The assessment and treatment of burn wounds requires a knowledgeable interprofessional health care team. Burn injuries can range in depth from a minor superficial injury to a deep full-thickness wound that may include the underlying structures and organs. All depths of injuries require a multifaceted plan of care to prevent infection, scarring, contractures, and death. The plan begins with an in-depth assessment of the injury to determine its effect on organ function and subsequent morbidity and mortality. After airway and hemodynamic stabilization, wound care is the first priority to ensure survival of the patient. Wound infection can potentially lead to deeper tissue injury and the development of life-threatening sepsis. Therefore survival depends on effective management of the wound from the time the patient is admitted until discharge.
Clinical Problem
Burn wounds can range from a minor superficial injury to a deep full-thickness wound that may include the underlying structures and organs. Burns are classified as minor, moderate, or major, depending on the total body surface area (TBSA) involvement, the depth of the injury, and the age of the patient. All three categories of injury may cause a systemic response including shock, but the deeper and more extensive injuries have a greater incidence of the life-threatening systemic reaction. Therefore an immediate and ongoing daily assessment of the burn wound is essential in preventing complications and ensuring a full recovery.
Burn Wound Assessment
The initial admission assessment of a burn wound includes determining the:
- •
etiology
- •
time and place the injury occurred
- •
causative agent
- •
depth of injury (partial vs full thickness)
- •
TBSA
- •
area of body
- •
age of patient
- •
past medical history
- •
risk factors that affect wound healing
- •
part of the body burned
The treatment plan is based primarily on the information from this assessment. For example, fluid resuscitation calculations are based on the time the injury occurred, the size and depth of the injury, the patient’s past medical history, and age of the patient. If the injury occurred in an enclosed space, there may be inhalation injuries.
Etiology
Burn injuries occur when the skin comes into contact with steam, flames, radiation, chemicals, electricity, or gas. Knowing the cause of the injury and the length of exposure helps determine the depth of the injury and the treatment plan. For example, if the causative agent is chemical, this may need to be emergently neutralized to stop the burning effect.
Electrical Burn Injuries
Electrical burns present a unique set of issues in that they tend to be deeper than most burn injuries. The depth and severity of the injury depend on the voltage, length of exposure, and the pathway of flow. It is difficult to assess the extent of damage accurately because much of the damage occurs internally as the electrical current travels along the tendons and vessels, creating deep wounds that often extend into the subcutaneous tissue and muscle fascia.
Inhalation Injury
It is essential to know the environment where burn injury occurred to determine the risk of inhalation injury. If the burn occurred in an enclosed space, such as a house or a car, there is a significant risk for inhalation injury even in the absence of cutaneous injury. Inhalation injuries are serious and the leading cause of fire-related deaths. When smoke inhalation injuries are combined with cutaneous injuries, the mortality rate increases significantly. These injuries present a unique set of problems, one of which is difficulty in diagnosing the full extent of the injury. Criteria used to evaluate the likelihood of inhalational injury include:
- •
The injury occurring in an enclosed area
- •
Burns to the face and neck
- •
Singed nasal hairs; a hoarse, dry cough; bloody/sooty sputum; and labored respirations
- •
Edema, blisters, and ulcerations along the mucosal lining of the oropharynx and larynx that increase for 24 to 48 hours after the injury
- •
Increased rate and depth of respirations
- •
Respiratory distress
- •
Confusion and decreased level of consciousness
- •
Stridor
- •
Decreased oxygen saturation levels
Nursing care in cases of inhalation injury includes:
- •
Suctioning
- •
Raising the head of the bed
- •
Monitoring of oxygen saturation levels
- •
Assessment of the need for intubation and mechanical ventilation
Injury Depth
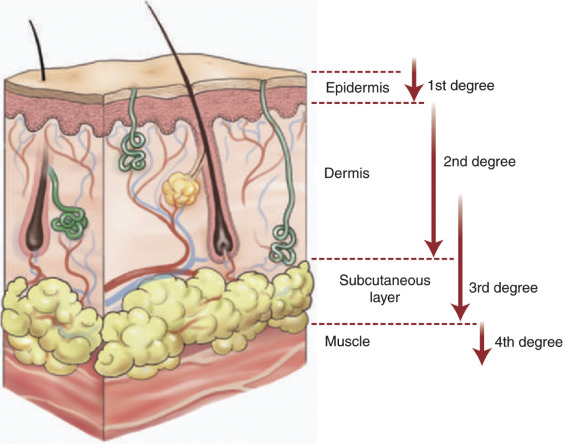
The depth of a burn injury is an important predictor of morbidity and mortality. It also determines the surgical management along with functional and cosmetic outcomes. Burn depth is expressed in terms of partial-thickness and full-thickness injuries. Both partial-thickness and full-thickness injuries can vary in depth. Partial-thickness injuries can be superficial, involving only the epidermis, or may extend into part of the dermal layer. Partial-thickness injuries have enough intact epithelial cells, hair follicles, and sweat glands to provide a new epidermis. Full-thickness injury results in the destruction of all skin layers, and there may also be destruction of subcutaneous tissue, muscles, and bones. Fig. 4.2.1 outlines the layers of tissue and demonstrates the difference in depth between a partial-thickness injury and a full-thickness injury.
Superficial Partial-Thickness Wounds
Also referred to as first-degree burns, these wounds appear red, may have localized edema, blanch with pressure, and have no blister formation. The wound may be firm if there is edema, and these wounds are painful. Wound healing occurs spontaneously in a few days to possibly 2 weeks and usually causes no cosmetic or functional impairment.
Deep Partial-Thickness Wounds
Also referred to as second-degree burns, these wounds appear pink or dark pink, white, tan, or cherry, are firm and blanch with pressure, typically have large thick-walled blisters, and are painful. Healing occurs spontaneously in about 3 weeks. Fig. 4.2.2 is a partial-thickness injury. Infection, trauma, and a decreased blood supply increase the risk of a partial-thickness injury converting to a full-thickness injury.
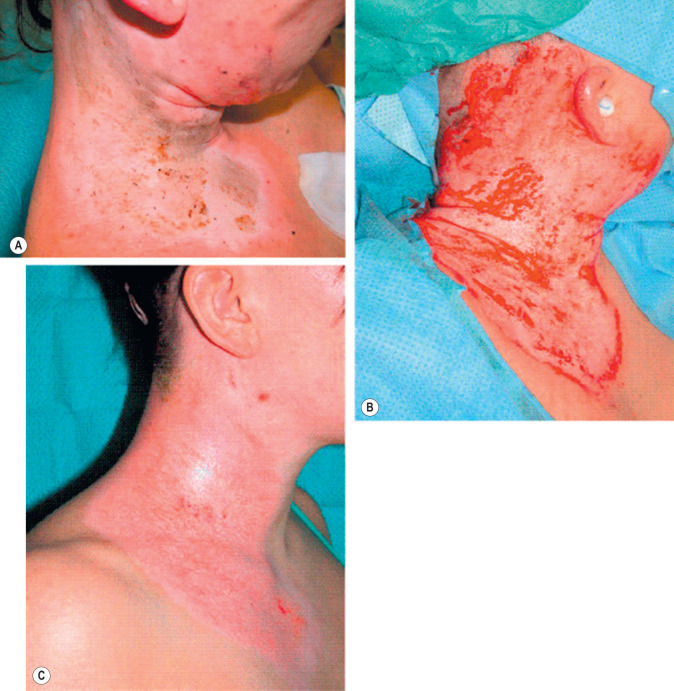
Full-Thickness Injuries
Also referred to as third- and fourth-degree burns, these wounds appear dark red, white, black, gray, tan, or waxy, and have no blanching or sensation to pain on light touch because the pain and touch receptors have been destroyed. Blister formation is minimal, if present, and blisters are thin-walled and do not increase in size. Closure of the wound occurs by granulation, epithelial migration, contracture, and/or surgical intervention. Figs. 4.2.3A and B are full-thickness injuries, and Fig. 4.2.4 is a full-thickness injury that extends down to the bone.


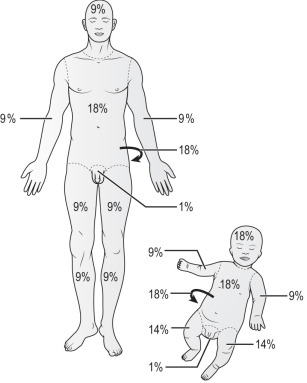
Size of Injury
The estimate of burn size is expressed as a percent of TBSA. A common, easy-to-remember formula for estimating percent of body burned is the Rule of Nines. The adult body is divided into seven areas, each of which represents 9%, or multiples of 9%, of the TBSA. For an adult, the head and neck equal 9%, the arms equal 9% each, the lower extremities are 18% each, the trunk is a total of 36% (18% anterior, 18% posterior), and the perineum is 1%. Thus the total is 100%. The percentage of body surface is affected by age and growth and development. Fig. 4.2.5 outlines the Rule of Nines for both adults and children.