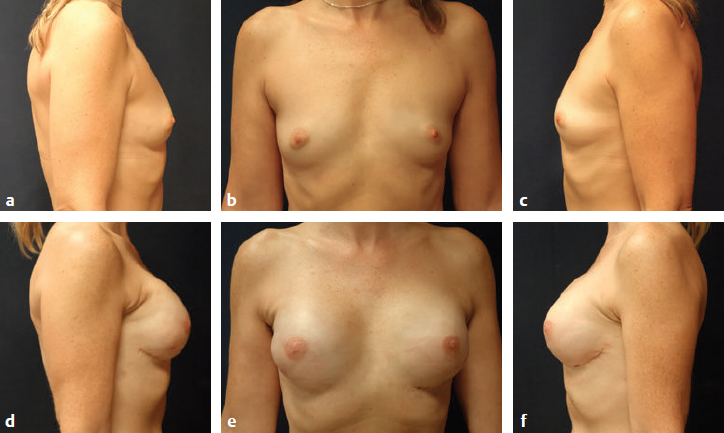
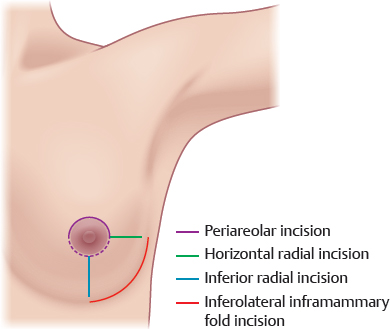
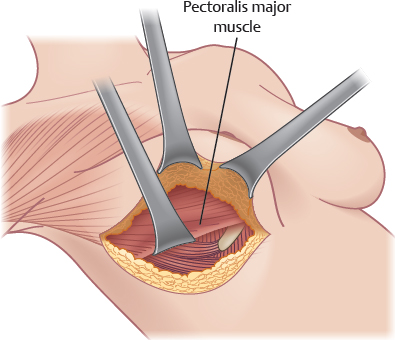
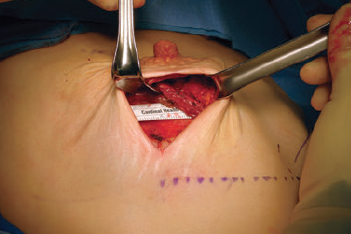
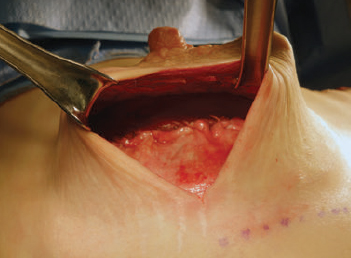
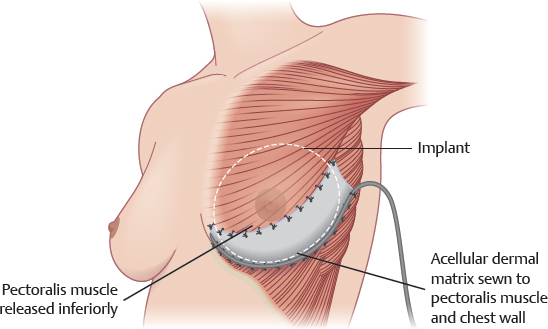
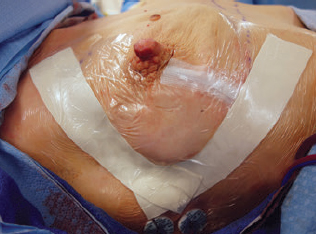
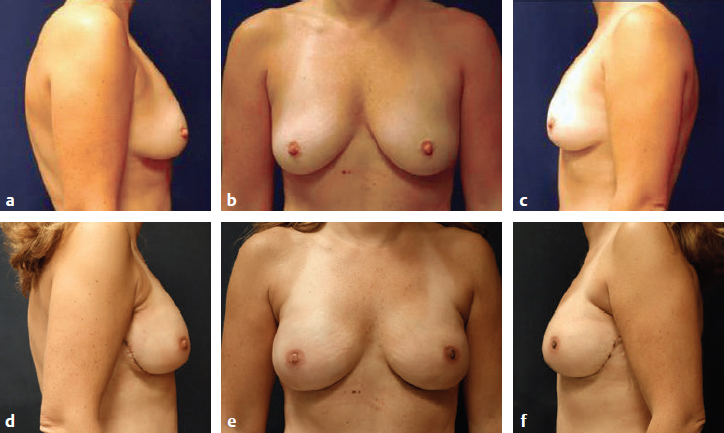
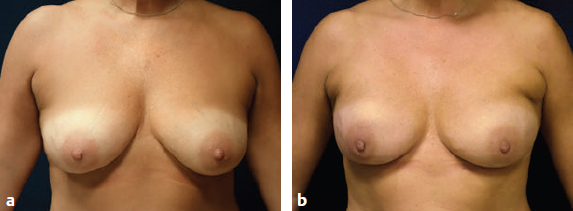
CHAPTER Implant reconstruction is the most common means to rebuild the breast in the United States. There has been a paradigm shift in the past 10 years, with more patients choosing mastectomy and bilateral mastectomy over lumpectomy and implant instead of autologous reconstruction.1,2 The reasons for this shift are multifactorial and include the enhanced ability to create reconstructions that closely resemble the native breasts. Improvements in mastectomy technique with skin and nipple preservation and refinements in reconstruction with partial muscle release and acellular dermal matrix (ADM) have contributed to the improved overall result.3–5 Despite advances in techniques, implant-based breast reconstruction has one of the highest rates of infection and complications of any procedure in plastic surgery.6–8 With mastectomy, the breast skin vascular supply is compromised, and in this compromised setting a foreign body is introduced. However, implant reconstruction is largely successful and has the advantage of a quicker recovery compared with autologous reconstruction with no donor site morbidity. A thorough understanding of surgical technique and the potential for complications or unfavorable results can reduce risks and help minimize avoidable mistakes. This chapter discusses surgical planning and technique for breast reconstruction with implants, identifies possible untoward events, and provides a template for management and prevention. Summary Box Complications and Unfavorable Results in Breast Implant Reconstruction Immediate/Early Late • Skin necrosis/nipple necrosis • Delayed healing • Erythema • Infection • Seroma • Hematoma • Dehiscence or exposure • Suboptimal shape • Implant malposition or inadequate size • Nipple malposition • Capsular contracture • Implant rupture • Animation deformity • Keloid or hypertrophic scar • Upper pole deficiency or divots • Implant rippling • Implant malposition or inadequate size • Symmastia or overdissection of the medial border • Suboptimal shape • Chronic pain Planning for implant reconstruction starts at the initial consultation. General health is assessed with age, BMI, and comorbidities. Whether the mastectomy is for cancer or prophylaxis can influence decisions on nipple preservation, laterality, and adjuvant treatment with chemotherapy and/or radiation. Specific attention is focused on identifying risk factors for implant failure. Active smoking, morbid obesity, uncontrolled diabetes, anticoagulation, and immunosuppression all pose challenges to reconstruction and in some cases require no or delayed reconstruction for patient safety (Box 38.1). Patients who are actively smoking at the time of consultation are strongly encouraged to quit. If still smoking at the time of surgery, these patients must understand that immediate reconstruction may be deferred until a later time depending upon how the skin responds to the mastectomy. I will not use ADM in active smokers and would only consider two-stage tissue expander–implant reconstruction with near-total muscle coverage or delayed reconstruction. Morbidly obese patients pose challenges for both implant and autologous reconstruction in relation to risk profile and overall cosmetic result. Immediate one- or two-stage surgery is considered on an individual basis depending upon the quality of the mastectomy skin envelope. Similarly, uncontrolled or severe insulin-dependent diabetes and immunosuppression increase the risk of complications. Modest immunosuppression from neoadjuvant chemotherapy is typically not considered a contraindication to immediate breast reconstruction, but transplant recipients on chronic immunosuppressant regimens require delayed or no reconstruction. Active therapeutic anticoagulation with coumadin or unfractionated or low-molecular-weight heparin poses too high of a risk for bleeding to consider immediate reconstruction if it cannot be suspended perioperatively. The physical examination records important anatomic landmarks, including notch–nipple, nipple–fold, and breast-base width dimensions. Overall breast and inframammary fold (IMF) symmetry is noted. An estimation of breast volume is assessed to ensure the correct implants and/or expanders are available at the time of the surgery. Routine lab values are obtained. A nasal swab to assess the skin flora is considered for health care workers, recently hospitalized patients, or those receiving neoadjuvant chemotherapy.9 The flora in these patients may include methicillin-resistant Staphylococcus aureus (MRSA) or gram-negative rods. These would not be covered in routine perioperative antibiotic administration. • Active smoking • Morbid obesity • Uncontrolled diabetes • Anticoagulation • Immunosuppression An increasing proportion of mastectomies are nipple-sparing. The surgical oncologist decides whether the patient is a candidate for nipple preservation based on the oncologic risk, and the plastic surgeon then decides whether it is a good idea aesthetically. Patients with grade I or grade II ptosis are often good candidates for nipple-sparing mastectomy (NSM). Breasts with grade III ptosis or very large breast size are assessed on an individual basis with considerations for premastectomy staged mastopexy or a two-stage tissue-expander implant reconstruction using an inferior vertical approach. For NSM, incision placement is planned with the surgical oncologist4 (Fig. 38.1). A lateral radial incision optimizes blood supply to the nipple and may therefore be optimal for those inexperienced with the technique. An inferolateral IMF incision optimizes cosmesis.10 The incision starts at approximately the 6 o’clock position and extends to the 3 or 9 o’clock position. Therefore the incision becomes longer with increased breast size. This is advantageous for removing the upper pole breast tissue and also for axillary lymph node sampling. The incision curves along the natural border of the breast and is thus hidden. With experience, this incision minimizes the risk of complications, which may be related in part to the increasing thickness of breast skin as it nears the abdominal transition. Full-thickness periareolar incisions are avoided because of the higher risk of nipple necrosis. As previously mentioned, an inferior vertical incision is chosen for ptotic breasts for greater uplift and improved nipple centralization. If nipple preservation is not possible, skin-sparing or skin-reducing incisions are planned according to current and desired breast size. Incisions may be oriented transversely or vertically depending upon the width of the breast and anticipated axillary extension. Although the Wise/inverted-T skin pattern optimizes cosmesis for large breasts, it is associated with a higher rate of complications. The gold standard of implant reconstruction remains a two-stage approach with a tissue expander followed by exchange with an implant at a second surgery. However, there is increasing interest in direct-to-implant (DTI), single-stage reconstruction.11 With DTI, the final implant is placed at the time of the mastectomy, which obviates a secondary surgery to replace a temporary expander. Patients are considered candidates for DTI if their goal is to stay about the same size. The best candidates are nonsmokers within normal weight range who are also relatively symmetrical and overall healthy. A reliable breast surgeon is critical to the success of DTI reconstruction. Patient preferences also strongly influence whether one- or two-stage surgery is performed. The final decision is made at the time of surgery after the mastectomy and depends on how the breast skin responds to the mastectomy. Fig. 38.1 Common incisions used in nipple-sparing mastectomy. Full-thickness periareolar incisions are typically avoided because of the increased risk of complications. (Modified from Colwell AS, Tessler O, Lin AM, et al. Breast reconstruction following nipple-sparing mastectomy: predictors of complications, reconstruction outcomes, and 5-year trends. Plast Reconstr Surg 2014;133(3):496–506.) The advent of ADM offered the ability to release the pectoralis muscle inferiorly, thus creating a pleasing breast contour, while avoiding pectoralis muscle retraction and implant malposition laterally or inferiorly (bottoming out). The first and most commonly used ADM is human ADM. Human ADM is very malleable, thus contouring to the implant, yet it retains the strength necessary to uphold implant reconstructions. It yields another advantage of long-term soft tissue support, which most patients undergoing a mastectomy benefit from. A number of other products have been developed from porcine dermis, fetal bovine dermis, and synthetic products such as silk or Vicryl. ADM is used for most one- and two-stage reconstructions, although some surgeons still prefer two-stage reconstruction with total or near-total muscle coverage. The advantage of total muscle coverage includes a potentially lower risk of complications, because the muscle covers the expander, but the disadvantage is difficulty in achieving a natural shape and in performing DTI reconstruction. Fig. 38.2 After mastectomy, the skin is evaluated for perfusion and thickness. In this patient, the color of the skin appears completely normal and the skin thickness appropriate for her size, with a mottling of subcutaneous fat. The IMF is marked on each breast, and its relation to the opposite breast is noted for symmetry. The incision is marked with input from the surgical oncologist. A paraver-tebral block gives significant analgesia during the surgical procedure and for the next 24 to 36 hours. If resources are available, this block can be offered to all immediate implant reconstructions. Before induction, pneumatic compression devices are placed and intravenous antibiotics are given. The anterior chest, and extending laterally to the operating room table, is prepped with chlorhexidine or iodine povacrylex, and sterile drapes are placed. Once the mastectomy is complete, the patient’s skin is reprepped with chlorhexidine, avoiding the open incisions. New sterile drapes are placed over the existing drapes. The patient’s arms are angled approximately 75 degrees from the operating room table, and muscle paralysis is used in conjunction with general anesthesia to facilitate subpectoral muscle dissection. The skin is inspected for color and overall thickness (Fig. 38.2). A blue-gray hue, exposed dermis on the undersurface, button holes, or excessive thinness of the skin flap predict ischemia. If present, a DTI procedure should typically be avoided and delayed reconstruction contemplated. Notably, the thickness of the flap alone cannot be relied upon as the only marker of the quality of the skin flap, because traction and cautery injury manifest as changes in the color of the skin rather than in the overall thickness. It may seem logical that very large breasts would have ample skin to work with and thus make them ideal DTI candidates. However, often the skin is more compromised in these patients, which may be related to the distance the blood needs to travel to cover the entire anterior breast surface and to the traction injury that may occur when removing the large volume of tissue. The pectoralis muscle is released from its lateral edge to the medial sternal attachment using electrocautery. Care is taken to coagulate the vessels with electrocoagulation in two places and perform division in between. Inferiorly, the pectoralis muscle is typically divided approximately 1cm above its attachment to prevent disruption of the IMF, if intact. Dissection proceeds medially until the 4 or 8 o’clock position on the chest wall (Fig. 38.3). This extent of dissection is necessary to avoid lateralization of the implant. Further dissection can be performed, but this results in more subcutaneous coverage of the implant and requires a larger piece of ADM. The lateral border definition for most mastectomies is the anterior border of the latissimus dorsi muscle, which is significantly more lateral than the desired border of the new reconstruction. The width of the new breast pocket is designed approximately 1 cm more narrow than the desired implant to account for the stretch inherent in human ADM (Fig. 38.4). If alternative stiffer products are used, the dimensions may more closely resemble the base width of the implant. For DTI, the implant volume is estimated based on breast-base width, breast weight, and desired postoperative size. For NSM, a small increase in the size of the implant typically fits the skin envelope the best, whereas in skin-sparing mastectomies a small decrease in size is often necessary. Fig. 38.3 The pectoralis muscle is released inferiorly to allow a natural breast shape with tissue expander–implant or direct-to-implant reconstruction. The pectoralis muscle is released to the 4 or 8 o’clock position to allow the implant to fit under it. A tissue expander is chosen to match the breast width, with nipple centralization for NSM, and to accommodate the desired increases in breast volume. I prefer to sew the ADM to the chest wall as the initial step, and subsequently to tailor the ADM–pectoralis muscle border with the implant in place. The rectangular or contoured ADM is oriented in place in the pocket. I prefer permanent sutures (0 Ethibond) for the ADM–chest wall stitches and absorbable sutures from the ADM to the pectoralis muscle (2–0 Vicryl), although some authors prefer absorbable sutures for both. Permanent sutures may be advantageous for defining a new IMF or lateral breast border. The ADM is first stitched medially to the released border of the pectoralis muscle. It is important to leave some redundancy medially to accommodate the implant. A tight medial pocket will serve to push the implant laterally. The second stitch is sewn to the IMF to prevent medial constriction, and the subsequent sutures are then sewn to the chest wall. If the IMF is intact, the ADM can be sewn to the fold; however, round implants will drop 1 to 2 cm postoperatively; shaped implants will also drop, but not to the same degree. If the IMF is not intact and the ADM is sutured to the skin flap, this will lead to bottoming out. As the pocket proceeds laterally, horizontal mattress sutures are placed from the ADM to the serratus muscle, avoiding redundancy. A medial and lateral stitch from the ADM to the pectoralis muscle is then placed along with a sizer. The most commonly used sizers are disposable saline sizers. Although the sizers do not exactly match the look of the silicone implants, they approximate it well, and with experience predictable results are achieved. Silicone sizers are available but cost more, and many institutions do not have the correct equipment for their sterilization for multiple uses. A sizer is sewn into the pocket with a U-stitch to keep it in place. The skin is stapled shut and the patient is positioned upright to check symmetry and pocket dimensions and for the final decision-making steps for DTI (Fig. 38.5) As the sizer is inflated, significant red or blue discoloration indicates the skin cannot withstand a full-sized implant, and a decision is made to place an expander or a smaller implant. Fig. 38.4 The pectoralis muscle is released to the 4 or 8 o’clock position. A ruler is inserted to the medial point of dissection, and a pocket is planned for the anticipated implant or expander. Fig. 38.5 A sizer is placed into the pectoralis–ADM pocket and sewn into place. The skin is stapled shut, and the sizer is inflated to the desired size. The pocket dimensions and skin color are observed during the inflation. The patient is then positioned upright to assess symmetry. Fig. 38.6 The implant or expander is placed into the pocket, and the pocket is closed using absorbable sutures. A tight fit is important for implants, whereas a slightly looser pocket is tolerated for expanders to accommodate the anticipated fill. Too loose a fit for expanders or implants can lead to bunching of the muscle and a step-off deformity. If available, objective measuring devices using indocyanine green (SPY, Novadaq) or other perfusion imaging modalities may help determine whether it is possible to place an implant and whether the skin will be viable. Although the exact cut-off numbers have not been determined for the SPY system, values in the low teens or significant drops in number with inflation of the sizer should be viewed with caution. The pocket IMF position and lateral border are viewed; it is important to have a hand-in-glove fit of the ADM with the lower pole breast skin. If the vertical dimension of the ADM is too short, the implant or expander will be pushed superiorly and/or flattened, and the breast skin may hang below the implant. This space is prone to seroma formation when the drains are removed, and the ADM will not be incorporated. Two drains are placed, with one running along the IMF and the other in the axilla and over the muscle. The exit sites should be tunneled 1 to 2 cm away from the breast pocket to allow and encourage closure soon after drain removal. Ideally these sites are placed above the position of the IMF so that they cannot be seen when the patient wears a swimsuit. However, the extent of lateral dissection with the mastectomy may preclude this. The pocket is first irrigated with dilute betadine solution, followed by two rinses of a triple antibiotic solution containing cefazolin, gentamycin, and bacitracin. These combinations have been shown to target the organisms most commonly involved in implant infections and implicated in the biofilm that may be related to capsular contracture. Hemostasis is achieved with particular attention paid to bleeding on the surface of the pectoralis muscle and in the axillary region. The surgeon’s gloves are changed, and the skin is washed with an antibiotic solution. During DTI, it is important to check that the patient remains paralyzed; otherwise it may be difficult to get the implant into the pocket, and the muscle will contract away with attempts to stitch it to the ADM. The implant or expander is then placed and the ADM is tailored and trimmed if necessary to give a tight fit to the implant. A tight fit will put tension on the muscle and help prevent a retraction contour abnormality; it will also help position the implant medially and help prevent lateralization and bottoming out12 (Figs. 38.6 and 38.7, Video 38.1). The expander is filled with a closed system consisting of a bag of saline and a three-way stopcock to deliver the saline to the expander (Fig. 38.8). The pocket is irrigated once again before closure. The skin edges are trimmed or deepithelialized. Deepithelialization has the advantage of leaving more dermal support and contact and can leave three solid layers to close with absorbable sutures. The incisions are then sealed with a surgical glue followed by clear adhesive dressings. Biopatches (Johnson & Johnson) are impregnated with chlorhexidine and are used around the drains to help prevent drain-site infections. Microfoam tape is often applied laterally to push the implant more medially and minimize the suction deformity that can be caused by the drain, which may lie close to the medial border of the pocket (Fig. 38.9). This is also covered by clear adhesive dressings to allow the patient to shower postoperatively. Fig. 38.7 Acellular dermal matrix acts as an extension of the pectoralis muscle to the chest wall. The inferior aspect of the pectoralis muscle is sewn to the acellular dermal matrix, which is sewn to the chest wall, creating a complete pocket around the implant. Fig. 38.8 A closed system is used to inflate the tissue expander for sterility. Fig. 38.9 Microfoam tape is often placed to help secure the lateral border of the implant or expander. Clear adhesive dressings cover the tape for showering and can assist in positioning the nipple. No bra is worn until postoperative day 1. At this time, a loose-fitting bra is used for some support. Compression garments should not be used, because they place too much pressure on the healing skin. While the patient is in the hospital, oxygen is administered by nasal cannula and is not weaned. Patients are discharged on postoperative day 1 or 2. Oral antibiotics are continued until the drains are removed, and medication is provided for pain control and muscle spasms. Activity and arm movement are restricted until the drains are removed. Arm range of motion is started 3 to 4 weeks after surgery, and strenuous exercise is avoided for 2 to 3 months. Implant massage is started at 4 weeks for round implants. Gentle massage can help prevent capsular contracture, whereas aggressive massage is avoided to help prevent implant malposition and rippling. If the patient has textured implants, no implant massage is recommended. For women working outside the home at a desk job, the average time off work is around 4 to 6 weeks. At 3 months, there are no restrictions. Figs. 38.10–38.13 show case examples. Fig. 38.10 (a–c) This 40-year-old woman had breast cancer of the left breast. (d–f) She underwent bilateral nipple-sparing mastectomy and direct-to-implant reconstruction using smooth round silicone gel implants. Fig. 38.11 (a) In a larger-breasted patient with ptosis, direct-to-implant reconstruction remains possible. (b) Although a vertical incision would have served to raise the nipple position to a greater degree, the inferolateral inframammary fold incision has the advantage of a hidden scar, which many patients find preferable, at the expense of a slightly lower nipple position.
38
Breast Reconstruction with Implants
Avoiding Unfavorable Results and Complications in Breast Reconstruction with Implants
Surgical Planning and Technique
Preoperative Planning and Considerations
Initial Consult
Incisions
Direct-to-Implant or Tissue Expander–Implant Reconstruction
Acellular Dermal Matrix

Surgical Technique
Skin Inspection
Partial Pectoralis Muscle Release
Pocket Creation

Implant Insertion
Closure

Postoperative Care
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine