Introduction
Breast reduction surgery is not only about improving the quality of life of women with the symptoms of macromastia but also improving the patient’s perception of her own image. Although it is thought by surgeons that the horizontal scar is the scar that bothers most patients, when 66 prospective patients desiring reduction were asked to rate line drawings and postoperative photographs of all three reduction techniques (Wise pattern, vertical, and no vertical scar), the no-vertical-scar operation was significantly preferred by the prospective patients. In addition to removing the vertical limb of the T scar, this procedure does not result in the disfiguring pull of the vertical limb on the shape of the new areola and significantly reduces the healing complications of the inferior T connection on a standard Wise pattern. The no-vertical-scar technique was brought to our attention by Passot and later re-popularized by Lalonde and Nagy.
The no-vertical-scar breast reduction is an excellent operation for specific groups of patients: (1) women with very pendulous breasts with the present nipple–areola complex at least 7 cm below the proposed new nipple–areola position, (2) patients who do not want a vertical scar, and (3) women with the same nipple position and in whom the risk of trifurcation loss is very high with a standard Wise pattern resection (e.g., obese, diabetic, immune suppressed, smoking history).
Indications and contraindications for the no-vertical-scar technique are as follows:
- •
Macromastia: Patients with large breasts desiring a reduction in size and who meet the criteria of having their present nipple positions at least 7 cm lower than the proposed new nipple position. Patients would prefer this operation if they are at high risk for delayed wound healing or wish to avoid the vertical scar.
- •
Breast ptosis: Patients relatively happy with their breast size but not happy with their shape because of excess skin sag, are a candidate for a mastopexy, would prefer to not have a vertical scar, and meet the criteria for the procedure.
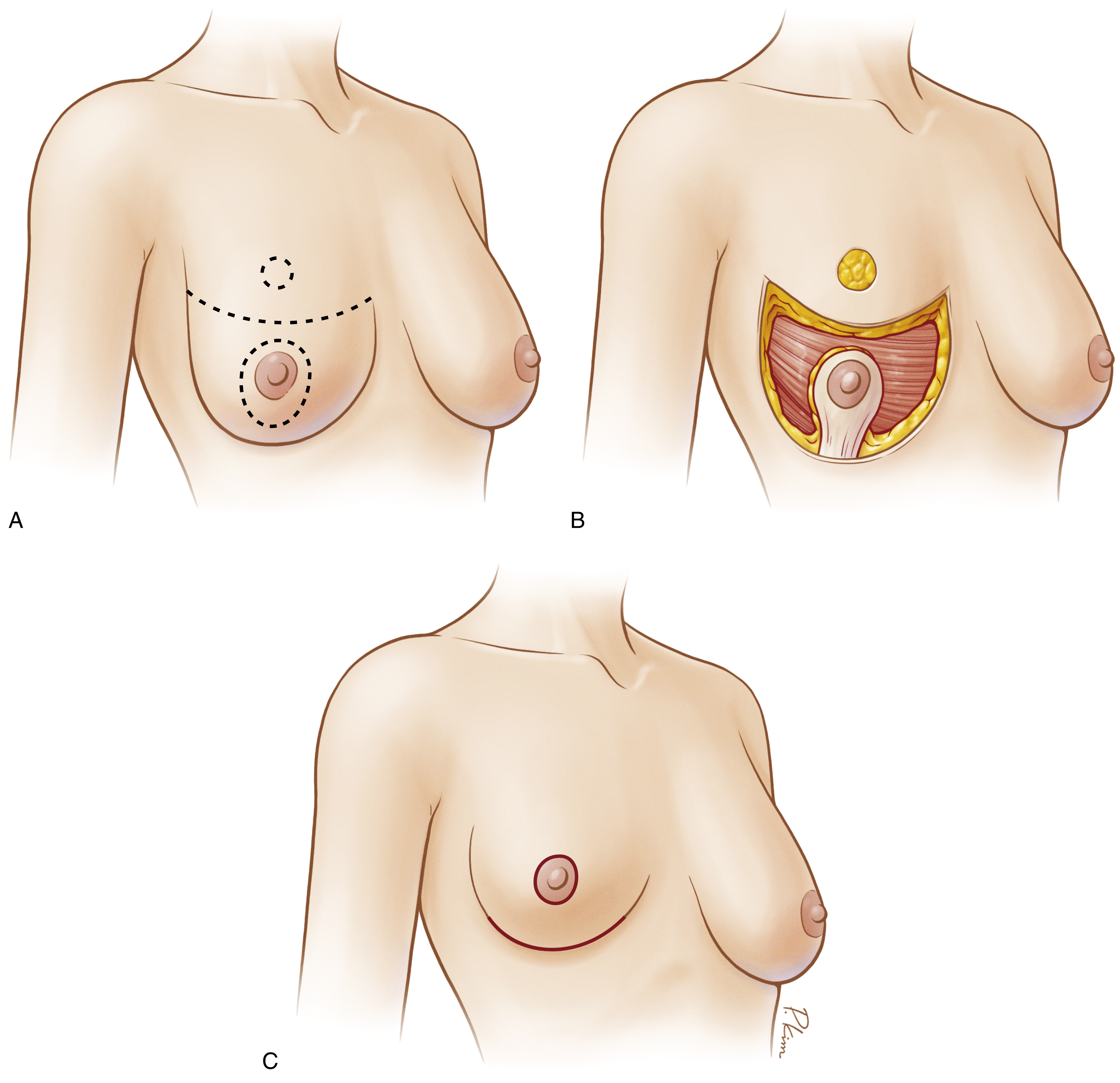
This procedure is available only to patients who have their present nipple–areola complex below the newly proposed horizontal incision ( Fig. 20.1A ). Dr. Lalonde demonstrates a way to reduce the need by 1–2 cm less, but this is not where you should start your experience. Patients must be healthy enough to undergo surgery and willing to accept the general risks of an inferior pedicle Wise pattern breast reduction.
Preoperative Evaluations and Special Considerations
It is important to discuss a woman’s family history of breast cancer and her breast health when considering any significant surgery on the breasts. These questions should start with age breast development started, whether the patient has had any pregnancies, age at first pregnancy, bra size before the pregnancy, size of breast during pregnancy and after delivery, present breast size, any breast masses identified and if biopsy was performed or mass removed, plans for more children, if future breastfeeding is important to the patient, and if the patient is at her ideal body weight or is planning weight loss. In addition to breast history, understanding the patient’s smoking history, diagnosis of diabetes or autoimmune diseases, present weight and plans for weight change, and any underlying cardiovascular disease; these will be important in your plans for the patient.
On physical examination, determining whether the patient is an appropriate candidate for a lift or reduction procedure, and, if so, how much tissue would be removed to obtain the desired breast volume postoperatively. An examination of where the new nipple position will be ( Figs. 20.2 and 20.3 ) and whether there is an adequate amount of transposition to have 5 cm of intact skin between the new nipple position and the upper limb of the skin incision ( Fig. 20.4 ) will determine if the no-vertical-scar technique can be used.



Surgical Technique
Relevant Surgical Anatomy
The most important anatomic aspect of breast reduction surgery is understanding the vascular blood supply of the patient’s breast and the planned operative pedicles. Any previous breast surgery could have injured the blood supply to the patient’s nipple or pedicle.
In the no-vertical-scar reduction, I use the inferior pedicle flap. The blood supply to the inferior pedicle comes from the internal mammary artery, the intercostal arteries, and the external branches of the lateral thoracic artery. It is important to not undercut the pedicle to allow the vessels to travel to the breast and the nipple–areola complex.
Markings
With the patient in the upright position, I first mark in green the suprasternal notch and then the meridian of the breast on each side using a long tape measure. I then transpose the inframammary fold (IMF) to the anterior surface of the breast to mark the proposed new nipple position (see Fig. 20.2 ) and mark with green. A similar procedure is performed on the opposite breast (see Fig. 20.3 ). A measurement from the suprasternal notch to new nipple position is checked on each side, and a visual check on their position being level is performed.
A Wise pattern tool is used to mark the standard markings for an inferior pedicle technique. This should make you very comfortable with the markings. I then connect the inferior limb of both wings, which will be the upper limb of resection.
Surgical Procedure
Details of the Procedure
Pedicle Elevation
After general induction and intubation, Xylocaine 1% with 1:100,000 epinephrine is injected along the proposed incision lines. I verify the width of the pedicle based on the length of the pedicle and the final size goal after surgery. It is usually 8–12 cm wide. The breast is held in a taut position with a garrote, and the nipple–areola complex is marked with a 38-mm cookie cutter. The inferior pedicle is then de-epithelialized; holding the pedicle steady, it is developed and care is taken not to undermine the blood supply during dissection. Tissue is left medially for final breast shape fullness and the lateral and axillary area is more aggressively resected ( Figs. 20.5, 20.6, and 20.7 ).