Breast Cancer Recurrence—Strategies for Risk Reduction
Kirsten Edmiston
History
Breast cancer is the most common cause of cancer in women. Sixty-four percent will have local stage disease, 27% will have regional disease at presentation, both potentially curable (1). At a fundamental level, all the facets of breast cancer care from surgery to adjuvant chemotherapy/endocrine therapy and radiation are done to eradicate the tumor and minimize the risk of recurrence. Surgery at its most elemental, physically removes the tumor. So then, what surgical strategies can be used to further reduce the risk of recurrence?
One can think about recurrence in terms of local (in-breast) recurrence, regional recurrence (RR) with the ipsilateral axilla, and distant recurrence. The risk of systemic recurrence varies greatly from patient to patient based on:
Tumor biology
Individual tumor’s molecular profile with the presence or absence of cellular estrogen receptors (ERs), progesterone receptors (PRs), HER-2 neu proteins (HER-2). The molecular subtypes are defined as hormone receptor (either ER or PR) (HR)+/HER-2− (luminal A/B), HR+/HER-2+ (luminal HER-2), HR−/HER-2+ (HER-2), and HR−/HER-2− (basal or triple negative)
Grade
Proliferation index (KI67)
Genetic predisposition
Stage at presentation
Patient characteristics (menopausal status)
The treatment of the disease
The molecular subtype has been found to be an independent predictor of recurrence-free survival and overall survival but not in-breast recurrence (IBR) after mastectomy (Fig. 20-1) (2). Surgeons cannot control the tumor biology and the patient’s germline mutations at the time of presentation and only to a certain extent, the stage at presentation and patient characteristics. The surgeon has the greatest impact on local and regional recurrence through their surgical treatment.
Mechanism of In-Breast Recurrence
The risk of in-breast recurrence (IBR) after mastectomy is approximately 4.9% at 5 years (3). This is independent of whether the mastectomy is done as a skin-sparing mastectomy (SSM) or nipple-sparing mastectomy (NSM). The median time for the appearance of clinically overt local recurrence (LR) is 2 to 4 years, depending on stage. Most recurrences occur on the skin/subcutaneous tissue not the muscle. Unfortunately, LR after mastectomy is rarely an isolated event with most eventually developing metastatic disease. Failure of mastectomy to prevent IBR may be related to the minimal yet irreducible percentage of residual breast tissue and lymphatics either in the skin flaps, or chest wall. Additional breast tissue can be found outside the confines of the mastectomy—above the clavicle, within the axilla, posterior to the anterior axillary line, and extending down on the abdominal wall through the inframammary fold.
Presentation of a Local/Regional Recurrence
An LR after breast-conserving surgery (BCS) may present in several different ways. Patients most commonly present with a new palpable mass or area of thickening in the breast or a new mass in the axilla. They may also present with small superficial skin nodules, measuring from 3 to 5 mm on the chest wall or an area of retraction in the skin or nipple. Patients may also be asymptomatic with only mammographic or sonographic evidence of malignancy (i.e., areas of architectural distortion, new microcalcifications, or masses). Tragically, patients can present with fungating masses in the area of a previous lumpectomy (Fig. 20-2). Patients who have undergone mastectomy with autologous reconstruction may also present in similar fashion with a palpable mass, skin nodules, areas of retraction, or new skin erythema. The differential diagnosis in this patient population can include the development of a recurrence, progressive fat necrosis, a chronic seroma, scar tissue, fibrocystic change, breast edema, and
idiopathic postmastectomy vasculitis (Fig. 20-3). Biopsy of the mass or skin lesion is critical to determine the nature of the lesion.
idiopathic postmastectomy vasculitis (Fig. 20-3). Biopsy of the mass or skin lesion is critical to determine the nature of the lesion.
 FIGURE 20-1 Association of molecular subtype and overall survival and locoregional recurrence (LRR) in patients with T1–2 breast cancer and 1–3 positive lymph nodes who underwent mastectomy without postmastectomy radiation therapy. (Reprinted with permission from Moo TA, McMillan R, Lee M, et al. Impact of molecular subtype on loco-regional recurrence in mastectomy patients with T1-2 breast cancer and 1–3 positive lymph nodes. Ann Surg Oncol 2014;21:1569.) |
In terms of timing, an LR, RR, or secondary primary tumor can occur at any time after treatment. Patients with an LR or RR have a significantly higher risk of developing distant disease and poorer overall survival as compared to those without an LR or RR. Geurts et al. reviewed the nationwide population-based Netherlands Cancer Registry cohort of women who were treated with curative intent for breast cancer (4). They analyzed the occurrence and timing of both the first recurrence and subsequent recurrences in 9,342 patients. They also identified prognostic factors for both first and subsequent recurrences. Lastly, they identified consequence of these patterns for
surveillance. Recurrence occurred in 1,853 women (20%). A total of 1,343 (72%) patients first presented with a distal recurrence while 362 (20%) had LR and 148 (8%) had an RR. Subsequent recurrences were also most commonly distant (Fig. 20-4). They identified that most commonly patients locally recur during the second year after treatment. RR and distant recurrences rates remain relatively constant through 10 years of follow-up (Fig. 20-5A). The annual risk of LR peaked at 2 years (0.7% [95% CI 0.5 to 0.8]) and 8 years (0.4% [95% CI 0.2 to 0.5]). The annual risk of RR peaked at 2 years (0.3% [95% CI 0.2 to 0.4]) and then decline thereafter (Fig. 20-5B).
surveillance. Recurrence occurred in 1,853 women (20%). A total of 1,343 (72%) patients first presented with a distal recurrence while 362 (20%) had LR and 148 (8%) had an RR. Subsequent recurrences were also most commonly distant (Fig. 20-4). They identified that most commonly patients locally recur during the second year after treatment. RR and distant recurrences rates remain relatively constant through 10 years of follow-up (Fig. 20-5A). The annual risk of LR peaked at 2 years (0.7% [95% CI 0.5 to 0.8]) and 8 years (0.4% [95% CI 0.2 to 0.5]). The annual risk of RR peaked at 2 years (0.3% [95% CI 0.2 to 0.4]) and then decline thereafter (Fig. 20-5B).
 FIGURE 20-2 This is an 80-year-old who presented with a neglected local recurrence. The patient had previously undergone breast-conservation surgery. The diagnosis was confirmed with a shave biopsy. |
 FIGURE 20-3 This is a 71-year-old female who presented with diffuse erythema 5 years after a skin-sparing mastectomy with DIEP reconstruction. The differential diagnosis was recurrence versus vasculitis versus infection. Punch biopsy demonstrated a nonspecific vasculitic process. |
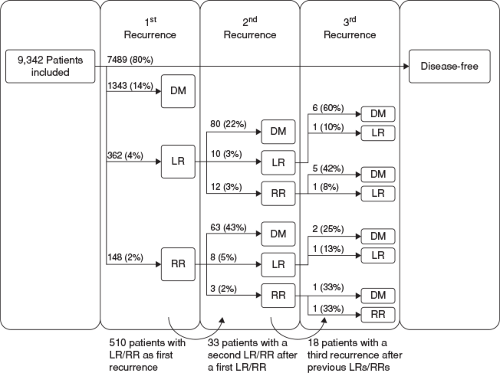 FIGURE 20-4 Flow chart of first and subsequent recurrences. LR, local recurrence; RR, regional recurrence; DM, distant metastasis. (Reprinted from Geurts YM, Witteveen A, Bretveld R, et al. Patterns and predictors of first and subsequent recurrence in women with early breast cancer. Breast Cancer Res Treat 2017;165(3):709–720. http://creativecommons.org/licenses/by/4.0/. No changes were made.) |
Estimation of Risk of Recurrence
Invasive Breast Carcinoma
Traditionally, risk of recurrence and treatment decision were based on clinical and pathologic staging, including tumor size, lymph node involvement, and the presence/absence of metastatic disease (TNM staging). Breast cancer (invasive and preinvasive) are now recognized to be heterogeneous with the outcomes based more on the individual tumor’s molecular profile with the presence or absence of cellular ERs, PRs, HER-2, and multiple other gene mutations. The most recent AJCC Staging Manual (8th edition) includes tumor characteristics, molecular biomarkers, and multigene panels that have been validated to have critical prognostic significance to prognostic staging beyond anatomic staging (5). With the inclusion of these molecular biomarkers and multigene panels, patients may undergo important and prognostic stage shifts. For example, in a subgroup analysis base on HR status, those with stage I to III, and HR− disease have a worse overall survival than those with HR+ disease (6). Overall, applying the 8th edition staging criteria resulted in a stage change for >35% of patients diagnosed with invasive breast cancer and refined overall survival estimates as compared to the 7th edition—6.8% were upstaged and 29.7% were downstaged.
Multigene Assays
Multiple multigene assays have been developed to assess recurrence risk and integrated into clinical care for both invasive breast cancer and DCIS. They differ in how they classify patients, leading to potential differences in treatment decision making and clinical utility.
Oncotype DX (Genomic Health, Redwood City CA) uses a 21-gene panel to stratify recurrence risk in patients with ER+ tumors with both N0 and N1 lymph nodes. The test uses reverse transcriptase-polymerase
chair reaction (RT-PCR) to measure expression of 16 cancer-related genes and 5 housekeeping genes. The involved genes are related to proliferation, invasion/metastases, ER, and HER-2 neu. Oncotype DX not only provides prognostic information but also helps to identify patients who would not benefit from chemotherapy. It has been incorporated in the American Society of Clinical Oncology (ASCO) and National Comprehensive Cancer Network (NCCN) and European Society of Medical Oncology (ESMO) guidelines along with the St. Gallen Consensus, and the NICE Diagnostic Guidance.
chair reaction (RT-PCR) to measure expression of 16 cancer-related genes and 5 housekeeping genes. The involved genes are related to proliferation, invasion/metastases, ER, and HER-2 neu. Oncotype DX not only provides prognostic information but also helps to identify patients who would not benefit from chemotherapy. It has been incorporated in the American Society of Clinical Oncology (ASCO) and National Comprehensive Cancer Network (NCCN) and European Society of Medical Oncology (ESMO) guidelines along with the St. Gallen Consensus, and the NICE Diagnostic Guidance.
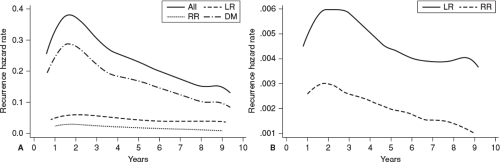 FIGURE 20-5 Hazard of (A) all first recurrences and (B) first LR and RR during 10 years of follow-up. LR, local recurrence; RR, regional recurrence; DM, distant metastasis. (Reprinted from Geurts YM, Witteveen A, Bretveld R. Patterns and predictors of first and subsequent recurrence in women with early breast cancer. Breast Cancer Res Treat 2017;165(3):709–720. http://creativecommons.org/licenses/by/4.0/. No changes were made.) |
Other assays that provide predictive information include MammaPrint that is useful for early-stage breast cancers and has the capacity to assess the risk of metastases to other body parts. Prediction analysis of microarrays 50 (PAM50) uses a 50-gene transcript to identify intrinsic breast cancer subtypes with prognostic impact. This assay is also known as the Prosigna assay that similarly uses intrinsic breast subtypes to determine a 10-year risk of distant recurrence in patients with early-stage ER+ breast cancer.
Recurrence Risk for DCIS
DCIS accounts for approximately 20% of all breast cancers diagnosed in the United States (7). The incidence of DCIS increased dramatically with the expanded use of screening mammography in women age ≥50 from the late 1980s until about 1998. Screening mammography increased from 29% of eligible women in 1987 to 70% in 2000. Since then, the incidence has increased at a much slower rate. Currently, the annual incidence of DCIS varies from 38 to 80/100,000 women, based on race, ethnicity, age, state residence, and breast density (1). Most recently in 2012 to 2016, the DCIS incidence rate is decreasing by 2.1% per year (8).
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
 Selection of Vascularized Lymph Node Donor Sites for Upper Extremity Lymphedema Surgery and Strategies to Minimizing Complications
Selection of Vascularized Lymph Node Donor Sites for Upper Extremity Lymphedema Surgery and Strategies to Minimizing Complications
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


