26
Botulinum Toxin: Cosmetic and Noncosmetic Dermatological Uses
Jaishree Sharad
Skinfiniti Aesthetic Skin and Laser Clinic, Mumbai, India
Introduction
Botulinum Toxin (BoNT) is an exotoxin derived from Clostridium botulinum, an anaerobic Gram‐positive bacterium [1]. In the late 1700s, poor sanitary measures in rural Europe’s food production during the Napoleonic wars (1795–1813) led to an outbreak of severe food poisoning‐related deaths in the community of Stuttgart [2]. The primary source was linked to the half‐cooked sausages which were being consumed during the wars, and the name botulism was coined for this disease (derived from the Latin for “sausage”) [3].
The first series of cases about BoNT poisoning was published in 1817 by J Kerner [4]. He postulated that the toxin developed under anaerobic conditions and acted by interruption of signal transmission in the peripheral nervous systems, the sympathetic, and parasympathetic nervous systems, leaving the sensory nervous system intact.
Belgian microbiologist Emile Pierre Marie van Ermengem of the University of Ghent identified C. botulinum bacterium in 1895 [5].
The pure isolate of BoNT A was isolated by Dr. Hermann Sommer from California in 1920 [6]. In 1946, Dr. Edward Schantz and his colleagues at the US Army campus were able to isolate large quantities of purified BoNT. In 1949, Arnold Burgen discovered that BoNT decreased the release of acetylcholine and blocked neuromuscular transmission [7].
Dr. Alan Scott, an ophthalmologist, found that small amounts of BoNT was able to correct strabismus in animal models [8]. Over a period of next two decades, Dr. Scott and Dr. Schantz collaborated to develop BoNT A for human use [9]. In 1978, the Food and Drug Administration (FDA) approved the batch for human use. In 1989, the FDA approved BoNT A for the treatment of involuntary muscle contractions, strabismus, blepharospasm, and hemifacial spasm.
Canadian ophthalmologist Jean Carruthers, in 1987, made an observation in her patients treated for blepharospasm with BoNT A. The frown lines had markedly disappeared. Together with her dermatologist husband Alastair Carruthers, she had discovered a treatment that would revolutionize the world of medical esthetics and antiaging treatments. In 1991, a pharmaceutical company called Allergan bought the research findings and renamed the agent as Botox™.
Physiology
All BoNTs are synthesized as single‐chain polypeptides with a molecular weight of approximately 150 kDa. All the serotypes have a particular amino acid sequence, all of which are known completely. All serotypes employ similar mechanisms of biological action as suggested by regions of sequence homology. Toxins have relatively little potency as neurotoxins in the single‐chain form. A two‐step modification in the tertiary structure of the protein is required for neurotoxic activation. In the first step, the parent chain is cleaved between amino acids 448 and 449. The result is one heavy chain (amino acids 449‐1295, approx. 100 kDa) and one light chain (amino acids 1‐448, approx. 50 kDa) connected via a disulfide bond. The light chain is associated with one atom of zinc [10]). The toxin enters the axon terminal in this form. Only after internalization by the target cell, the second activating step, i.e. disulfide reduction occurs [12].
The integrity of the disulfide bond is essential for BoNT’s biological activity [13].
The crystalline structure of BoNT type A is flat and comprises three modules: the endopeptidase (light chain), the translocation domain (N‐terminal half of the heavy chain), and the binding domain (C‐terminal half of the heavy chain).
BoNTs exert their activity through a multistep process that involves binding to nerve terminals, internalization, and inhibition of calcium‐dependent neurotransmitter release [14]
The heavy chain (~100 kDa) subunit of the BoNT molecule binds to receptors on nerve terminal membranes, located primarily but not exclusively on cholinergic neurons. The specificity of these receptors appears to be different between different botulinum serotypes [10, 15, 16]
Following binding, BoNTs are translocated into the neuronal cytosol via receptor‐mediated endocytosis. The exact mechanism of this translocation process is not known, but it has been speculated that the heavy chain can form a pore through which the light chain can pass [17]. Inside the endocytotic vesicles, the neurotoxin structure undergoes a conformational change in the presence of a low pH, and the light chain is released into the cytosol accompanied by reduction of the disulphide bond that linked it to the heavy chain.
Once inside the cytosol, the light chain cleaves one or more of the SNARE. SNARE is an Acronym derived from SNAP (Soluble Nethylmaleimide‐sensitive factor Attachment protein Receptor) proteins necessary for vesicle docking and fusion, thereby reducing exocytotic neurotransmitter release and preventing the release of acetylcholine into the synaptic cleft and reducing muscular and glandular activity.
Each serotype cleaves a specific peptide bond on one or more of the SNARE. BoNT A cleaves SNAP‐25 molecule. BoNT B cleaves synaptobrevin.
The enzymatic activity of the light chain requires the presence of the intramolecular zinc.
BoNTs act not only on efferent motor pathways but also on autonomic efferent pathways, which also utilize acetylcholine as a neurotransmitter. The inhibitory effects of BoNT type A on autonomic terminals have led to its successful use in conditions of autonomic hyperactivity such as hyperhidrosis and gustatory sweating.
Although the effects on autonomic and motor terminals are thought to occur by a similar mechanism (i.e. binding, internalization, and inhibition of neurotransmitter release), the clinical effects are of longer duration in autonomic conditions than in neuromuscular conditions. The reason for this difference is unknown.
Immunogenicity
BoNTs are biologic pharmaceuticals and can elicit an immune response like all foreign proteins. Some patients may develop IgG (immunoglobulin G) antibodies when BoNT therapy is continued over many years [18].
The BoNT A protein complex is formed of the core neurotoxin, responsible for its activity and the protective accessory proteins, called neurotoxin associated proteins (NAPs). Antibodies formed against the 150‐kDa core neurotoxin are capable of neutralizing its activity, but those formed against the nontoxic proteins in the BoNT do not affect its clinical efficacy.
Despite the antigenic nature of BoNT proteins, antibody formation that interferes with the clinical responsiveness to BoNT type A is infrequent. This is probably because of the high potency of BoNT type A, which produces clinical effects in extremely small quantities. However, frequent injections (i.e. more than every 12 weeks) or very high doses (>100 units) may increase the likelihood of an immune response against the neurotoxin.
There are very few studies which have attempted to determine the frequency of neutralizing or blocking antibodies against BoNT. Hence, the frequency is not known. While earlier studies are available on the immunoresistance of BoNT A, these are based on the original preparation of BOTOX which was in use until 1998. As per these studies, the frequency of antibodies reported is between 4.3% and 10%. The current BOTOX preparation contains 5 ng of neurotoxin complex protein per 100 units as compared with 25 ng in the earlier preparation. Thus the previous studies do not carry much importance.
Different BoNT A preparations vary in their antigenic potential. The antigenic potential load of Incobotulinumtoxin A, which contains only the 150‐kDa core BoNT without NAPs, is 0.44–0.6 ng/vial, compared to onabotulinumtoxin A and abobotulinumtoxin A which have an antigenic protein load of 0.8 ng/vial which suggest the least antigenic potentiality of incobotulinumtoxin. However, further studies are required to compare the antigenic potential of different products.
Other factors which affect the formation of neutralizing antibodies are
- Amount of inactive toxin in BoNT products: The 150‐kDa core BoNT of BoNT products is initially produced by the bacteria in an inactive form. This inactive toxin can stimulate antibody formation so the amount of inactive toxin in the BoNT product should be kept as small as possible.
- Accessory proteins: Most of the BoNT formulations contain NAPs, the function of which is to cover and sterically restrict access to the BoNT A site that is prone to the most neutralizing antibody formation. Thus the immunogenicity of neurotoxin products that are shielded by NAPs is very low.
- Previous exposure or vaccinations: Some patients who have received vaccination against BoNT to retain antibody titers to the neurotoxin, may not respond to the BoNT A. Thus, past history of vaccination or toxin is very important prior to treatment.
- Dose: Development of neutralizing antibodies to BoNT is directly proportional to the cumulative dose. Conditions which require lower BoNT A doses, like blepharospasm, hemifacial spasm, or for cosmetic indications, are reported to have lower rates of neutralizing antibody formation against BoNT compared with indications which require higher doses like torticollis or focal spasticity.
- Treatment intervals: Frequent BoNT injections given at shorter intervals (i.e. 12 weeks apart) increased the risk for neutralizing antibody formation, and later on patients may require higher doses than normal or may not respond at all.
Mode of Action
BoNT, when injected, blocks the neuromuscular junction [19].
This decreases the binding sites for the toxin. That is the reason that repeated injection into an already denervated muscle is not as effective, as uptake into the muscle is reduced. But this neurotoxic effect on the neuromuscular junction is temporary. After injection, the effect is evident within one to three days and maximal effect appears approximately two weeks after the toxin is introduced, then gradually declines after approximately three months.
Restoration of the neuromuscular junction occurs at two levels. In the axonal sprouting process, new neuromuscular junctions develop around the blocked terminal, but this is a temporary recovery process. These sprouts are removed when the original neuromuscular junction is restored.This inhibitory mechanism of action is also used in the treatment of hyperhidrosis. By its inhibitory action on the sympathetic fibers to sweat glands, where Ach is used as the neurotransmitter, BoNT is shown to effectively reduce sweat production.
Other indications for the use of BoNT are based on the fact that BoNT reduces the release of mediators of pain and inflammation. SNARE proteins, which are present within the vesicles located at sensory nerve terminals, release mediators of pain and inflammation, including substance P and cGRP (calcitonin gene‐related peptide). By blocking cGRP, glutamine, and substance P, BoNT A inhibits neurogenic inflammation and can ameliorate pain syndromes, such as migraine headache or psoriatic skin lesions.
Diffusion
Precise localization of the neurotoxin is important to achieve desired effects, because uncontrolled spread or diffusion of the toxin beyond the target muscle not only increases the risk of local and systemic effects but also makes the aesthetic outcome unpredictable and should be avoided [19, 20].
In the face, injection sites are very close to untargeted muscles, so it is important that the toxin does not diffuse into nearby muscles. Therefore, physicians should have knowledge of potential diffusion properties of each BoNT A formulation.
The release of acetylcholine at sympathetic nerve terminals stimulates exocrine glands to cause sweating. BoNT A, when injected, prevents the release of acetylcholine to cause temporary cessation of sweating. The area of anhidrosis produced is proportionate with the spread of the BoNT A preparation used. The larger the diffusion area, the greater the spread of the toxin, which might result in a larger area of reduced muscle activity. This property has commonly been used to study the diffusion of different botulinum preparation.
Trinidade de Almeida and colleagues conducted a study to compare the diffusion properties of BoNT A‐ona and BoNT A‐abo by injecting them on each side of the forehead and then analyzing the area of anhidrosis. Either side of each subject’s forehead was randomized to receive either BoNT A‐ona or BoNT A‐abo at two injection points (medial and lateral). The side of the forehead randomized to BoNT A‐ona received 3 U at each injection point. The alternate side was then randomized to receive an equal volume of injection of BoNT A‐abo but with a dose ratio of 1.0 : 2.5, 1.0 : 3.0, or 1.0 : 4.0. An iodine and starch test across the forehead was used to make the areas of anhidrosis visible. The halos of anhidrosis could then be measured and compared. In this study the injections were kept at constant volume regardless of the dose ratio. The anhidrotic halo for BoNT A‐abo was found to be larger at all dose ratios from week one to month six compared with the halos for BoNT A‐ona [21].
Studies which compared BoNT A‐ona and BoNT A‐inco showed that the complex proteins in BoNT A‐ona do not influence the diffusion profile and both had similar diffusion profiles. BoNT B consistently showed the highest local and systemic diffusion properties in various studies. The B serotype showed a greater radius of toxin diffusion and hence a higher number of associated side effects.
In addition to the type of BoNT, the other factors which affect diffusion include accurate muscle selection, dilution, volume, and dose injected.
Onset and Duration of Action
The effect of BoNT is temporary and reinjections are necessary once the effect wears off.
After Injecting BoNT:
- Onset of action – 12–72 hours
- Peak effect – 1–3 weeks
- Effect Plateau for – 2–3 months
- Effect wears off in – 3–6 months
Various studies have been done to detect the onset and duration of BoNTs. A study done by Carruthers to evaluate the efficacy of BoNT A‐ona (Botox) for the glabellar lines demonstrated that the maximal rate of response for frown lines lasted for three months in 75% of patients, and in 25% up to four months [22]. Similarly, a study using BoNT A‐abo (Dysport) with a 50‐U dose showed that the effect lasted anywhere from three to four months [22]
Thus for most aesthetic indications, the effect is seen within a week and lasts for three to four months, with patients often requiring reinjection approximately every four months [19] (except for masseter hypertrophy). In case of masseters, the maximal cosmetic benefit takes 6–8 weeks after injecting the BoNT and the result lasts for 8–12 months. Hence it is important to be aware of the expected time the patient has to be called for retreatment because it varies with different preparations and different indications.
Reconstitution and Storage
Various pharmaceutical preparations of BoNT are available in the market [23].
It is important to know about the various products before one chooses to do a treatment. In India, BoNT A (under the name BotoxR;Allergan) is available in vials of 50 and 100 units as vacuum dried neurotoxin complex which needs to be reconstituted with 0.9% preservative free normal saline for its usage. Dilutions of 1–10 cc have been suggested in various literatures. It is said that greater the dilution, the shorter the duration of effect and the higher the chances of diffusion.
However, in Dr. Klein’s survey, he found that a dilution of 2.5 cc per 100‐unit vial is what most of the experts use [24, 25].
Reconstitution of vacuum dried neurotoxin is done by filling 2.5 cc of saline into a syringe, then the needle is inserted gently into the 100‐unit vial. The plunger of the syringe should not be pushed because the vacuum in the vial itself allows the saline to penetrate into the vial. The vial should not be shaken vigorously in order to prevent foaming and bubbles, as this may result in denaturing of the neurotoxin complex. However, recent reports have shown that this is only theoretical and may not hold true in clinical practice [15, 23] (Figure 26.1).

Figure 26.1 Reconstitution of BoNT. [11]
The vial should be stored in a refrigerator at a temperature between 2 and 8 °C. An unopened vial can be stored for up to 36 months. However, once opened and reconstituted, the toxin retains its original potency for up to six weeks when refrigerated and in a frozen state for up to six months [26].
Patient Assessment and Selection
An appropriate patient selection is very crucial for a successful treatment outcome. Physicians should be thorough with the muscle anatomy. Before starting the procedure, the face should be evaluated for all dynamic and static wrinkles, as well as facial asymmetries. The asymmetries should be pointed out to the patient before starting the treatment.
Caution should be taken while treating older patients because in them the aging process is counteracted by using some other facial muscles, e.g. hyperfunction of the frontalis to overcome the ptosis of the eyebrows. Patients with excessive lower eyelid skin or lower fat pads should not be treated with BoNT as they will require adjunctive cosmetic procedures as blepharoplasty [27–29]. Patients, who extensively use the muscles of facial expression, such as actors, should be injected with low doses. A frozen expression can cost them their job.
The best candidates are those who have realistic expectations.
Pre‐Procedure Preparation
- Counseling a patient is the first step to a successful outcome. A thorough history and the proper examination is a must in order to understand the muscle anatomy of the patient’s face and to observe asymmetries if any. All contraindications should be ruled out.
The following points should be covered in counseling:
- The aim of the treatment should be to make the lines softer rather than trying to make the lines disappear. This will give a more realistic appearance.
- Only dynamic lines which are caused by contraction of the underlying muscle can be treated.
- Static lines and sagging of skin cannot be treated with BoNT.
Volumetric changes secondary to collagen degeneration such as deep wrinkles present at rest cannot be treated.
- The aim of the treatment should be to make the lines softer rather than trying to make the lines disappear. This will give a more realistic appearance.
Loss of dermal elasticity cannot be treated resulting in skin folds and wrinkles cannot be treated with BoNT.
- Dosage required. The doses differ in every individual as well as on both the sides of the face which depends entirely on the muscle anatomy, the muscle bulk and the asymmetries. After careful assessment, the required dosage and the cost need to be discussed with the patient.
- Scheduling the treatment. Timing of the treatment should be decided keeping patient’s activities in mind to give optimum results. Injection should be planned a week before the patient’s important event so that any corrections or touch ups required can be done. Never inject a patient who has an important event a day later.
- Result. Effects are usually visible by the second day post injection and maximum effect is achieved in a week. The treatment needs to be repeated between three and six months because the effect would wane by that time.
Preparing the Patient to Get Optimal Results
To prevent bruising, patient should avoid the following for a period of one week before the procedure:
- NSAIDS
- Gingko biloba/ginseng
- Green tea
- Vitamin E
- Glutathione
- Omega 3 supplements/fish oil
- Various herbal supplements which act as blood thinners
Patients on aspirin and other blood thinners due to medical ailments need to be cautioned that they may bruise and that the bruise may take a week or two to subside.
Consent and Photography
Documentation of any procedure is very important to avoid any legal issues. A written informed consent and photographs are mandatory. The consent form should include the type of BoNT to be used, the longevity, and the risk of possible complications. The consent form should also mention that the patient has no history of any contraindications for BoNT.
Photographs should be taken both in front and lateral profile views using a standard camera and good lighting. A clean background (white, black, or gray) is preferable. Photographs should be taken both at rest, to see static lines if any, and in motion i.e. asking the patient to make the necessary expressions. For example, take a picture after asking the patient to give a big smile in order to see the crow’s feet or to frown to notice glabellar frown complex. This will help to assess the anatomy of muscles at rest and at maximum contraction.
The Procedure
Before the procedure, topical anesthesia in the form of prilocaine or lidocaine may be used in patients who have a low threshold to pain. Ice packs can also be used in order to numb the skin. Talk therapy works most of the time. Before injecting, the area to be treated has to be clean with chlorhexidine sulphate and alcohol. The patient is asked to demonstrate various expressions and the muscles to be injected are delineated and the points to be injected are marked with eyeliner or a lip liner pencil.
The injection should be given while the patient is in a comfortable sitting position. 1 ml insulin or tuberculin syringes with 30–32 gauge needles should be used. Not more than 10 units per syringe should be filled to prevent pain due to blunting of needle with multiple punctures. Care should be taken not to overdose the patient, as touch up can always be done a week to 10 days later if required.
The Glabellar Complex and Vertical Frown Lines
The glabella is the area between the two eyebrows, and its contraction causes the appearance of two lines between the brows called the frown lines. Frown lines are associated with negative feelings such as anger, frustration, irritability, or worry [30].
The corrugators, procerus, depressor supercilii, medial fibers of orbicularis oculi and lower fibers of frontalis muscle are all responsible for hyperkinetic lines between the eyebrows, forming anesthetic vertical, horizontal, and oblique frown lines or wrinkles [31].
Glabellar lines may differ in appearance with gender (larger muscle mass and thicker skin in men), age, physical activity, solar exposure or ethnicity [32–36].
Muscles Involved
Procerus, Corrugator Supercilii, depressor supercilii.
In addition to these muscles, the medial fibers of the orbicularis oculi and the lower medial fibers of frontalis may interdigitate with those of the corrugator supercilii and contribute to frown lines. While making a treatment plan, one needs to take into account the interdigitation of muscle fibers and the degree to which their activities are in opposition to anticipate the effect of BoNT type A injection [37].
Procerus: This is a thin depressor muscle that pulls the medial part of the brow down causing horizontal wrinkles on the bridge of the nose. It originates over the periosteum of the nasal bone and inserts into the dermis of the glabella (Figure 26.2).
Figure 26.2 Anatomy of Corrugator supercilii and procerus muscle.
Corrugator Supercilii muscle: It originates at the medial supraorbital ridge of the frontal bone, runs obliquely in a superior lateral direction, and inserts in the skin, interdigitating with fibers of frontalis. It is deep centrally and gets more superficial at the point of insertion. It adducts and slightly depresses the eyebrow, thus moving it medially and inferiorly. Contraction of the corrugators causes vertical glabellar creases or frown lines (Figure 26.2).
Conventional Injection Technique, Sites, and Doses
The first point of injection is marked by drawing a line between the origin of the medial brow and the contralateral inner canthus on either side. The center of the procerus muscle lies at intersection of these lines [38]. Four to five units of botulinum are injected perpendicularly into the body of the procerus.
Two injection points are marked on the corrugators above the supraorbital ridge on either side. Dimpling of the skin on frowning denotes the insertion of the corrugator muscle and care should be taken to inject medial to this insertion point. It is also safer to stay medial to the mid‐pupillary line. Inject two to three units of neurotoxin, keeping the needle at a 45° angle. The lateral‐most injection should be superficial as the fibers of corrugators insert into the skin (Figure 26.3).
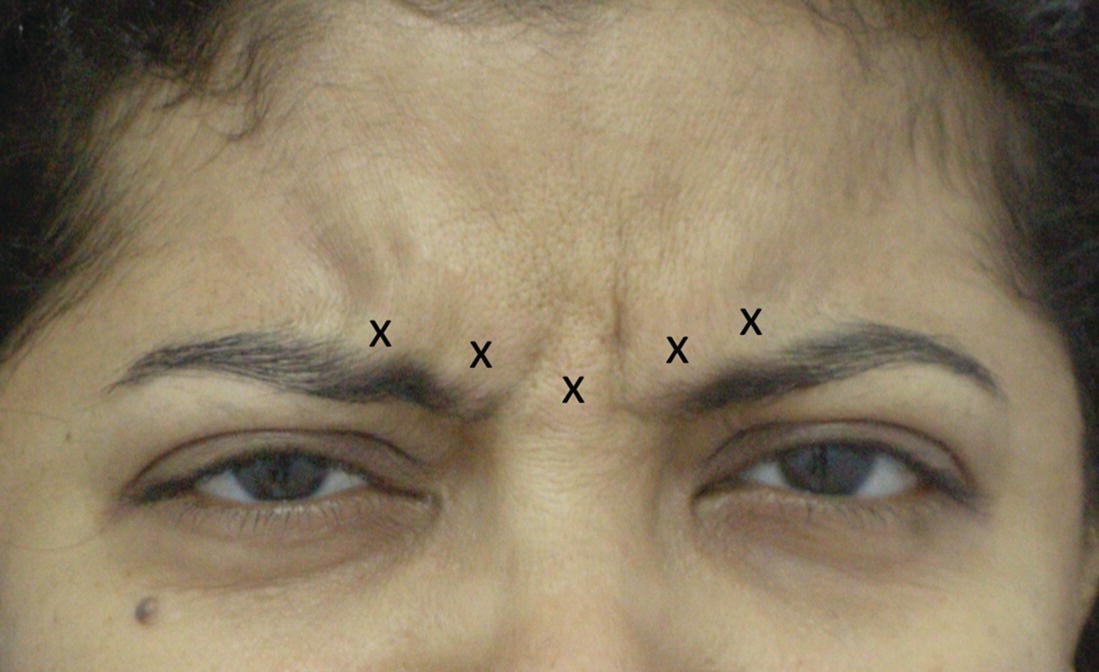
Figure 26.3 Injection points for glabellar frown lines.
Always place the thumb of the nondominant hand on the supra orbital ridge in order to prevent diffusion into the orbital rim.
It is better to be very conservative while injecting BoNT in elderly patients who may have a reduced or absent orbital septum. Large volumes, if injected, will increase the spread of the toxin from the injection site and hence the possibility of causing ptosis.
Two studies, one by Almeida et al. and the other by Kim et al., have shown five wrinkle patterns in the glabella region. These are described as
- “U” pattern (Figure 26.4a,b)
- “V” pattern (Figure 26.5a,b)
- “Omega” pattern (Figure 26.6a,b)
- “Inverted Omega” pattern (Figure 26.7a,b)
- “Converging Arrows” pattern (Figure 26.8a,b)
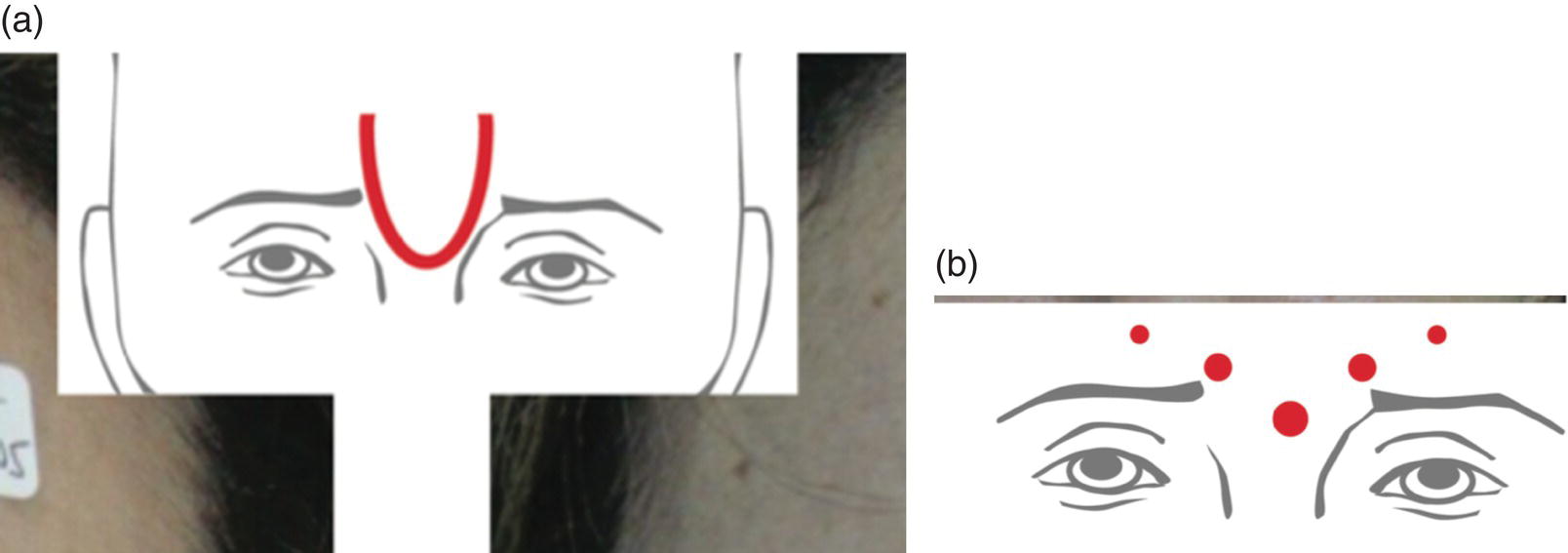
Figure 26.4 (a) Glabellar lines, U pattern. (b) Injection points for U pattern.
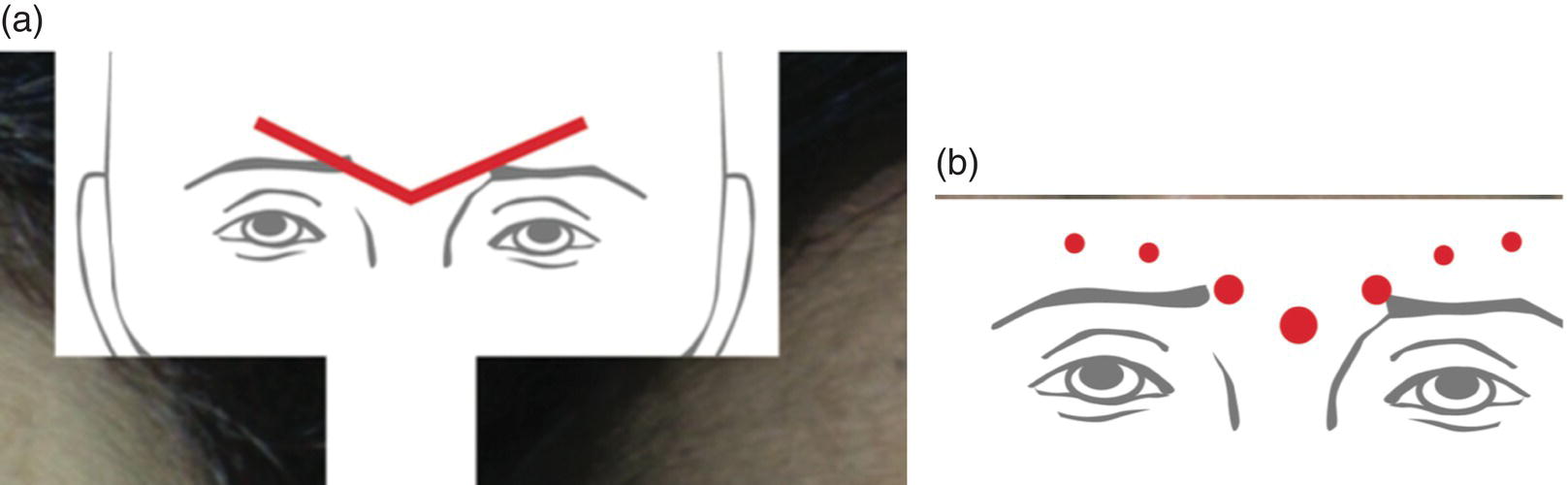
Figure 26.5 (a) Glabellar lines, V pattern. (b) Injection points for V pattern.
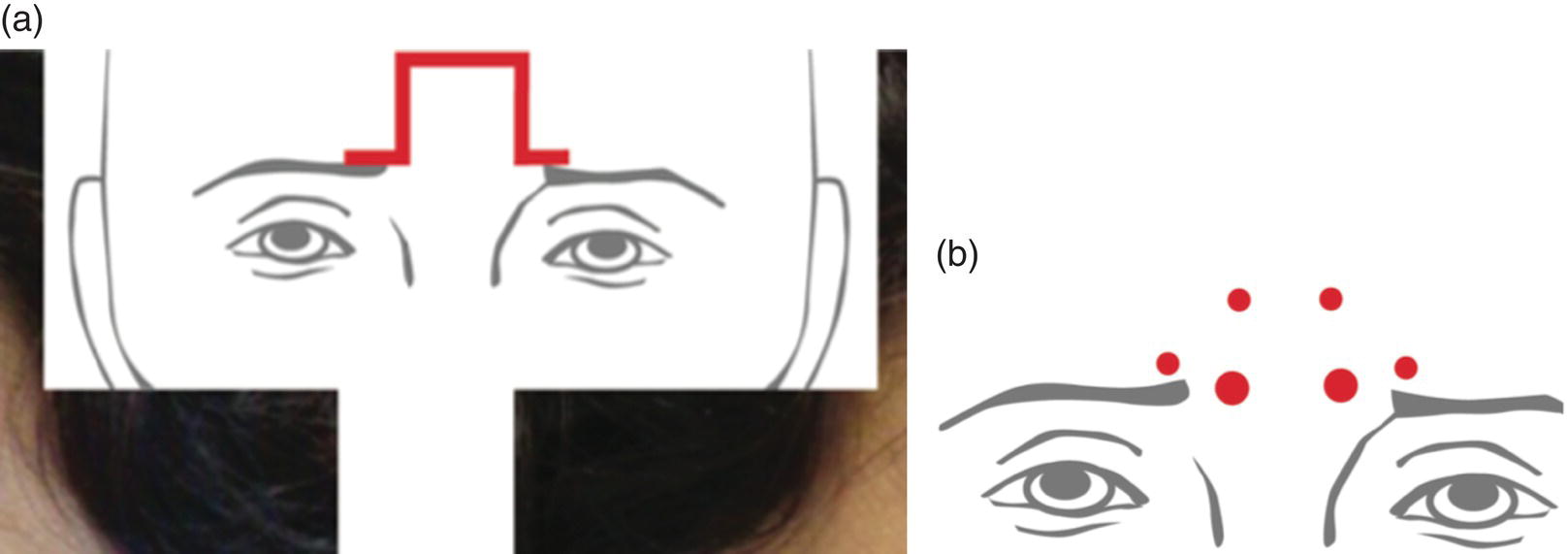
Figure 26.6 (a) Glabellar lines, omega pattern. (b) Injection points for omega pattern.
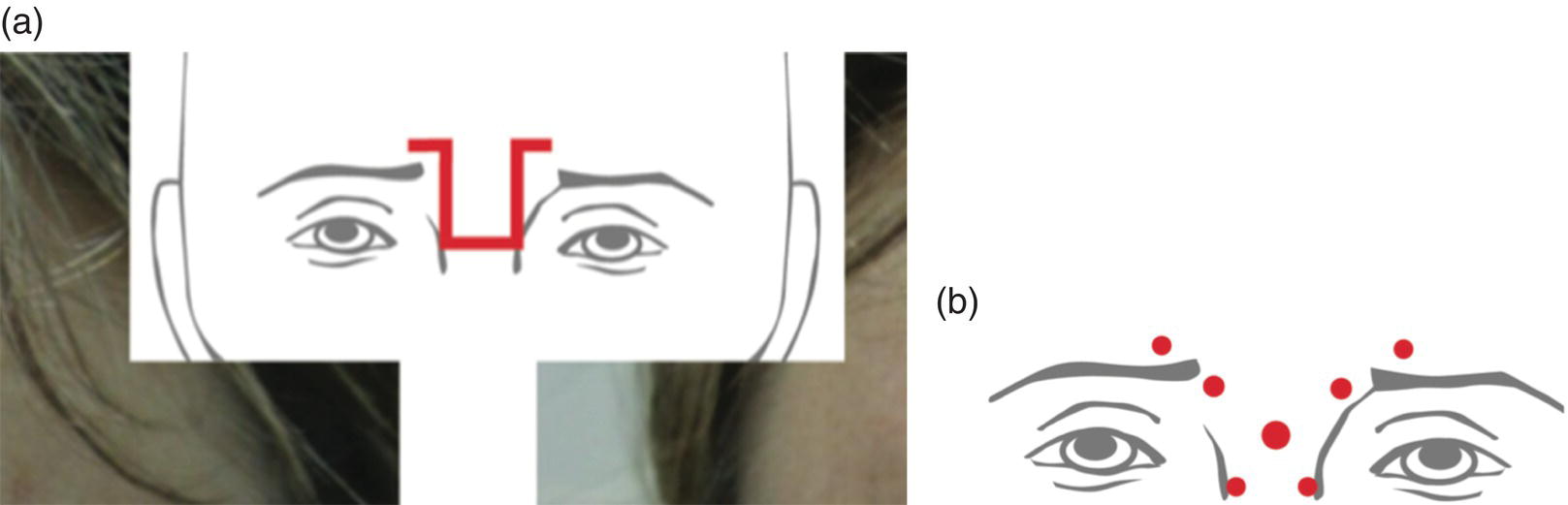
Figure 26.7 (a) Inverted omega pattern. (b) Injection points for inverted omega pattern.
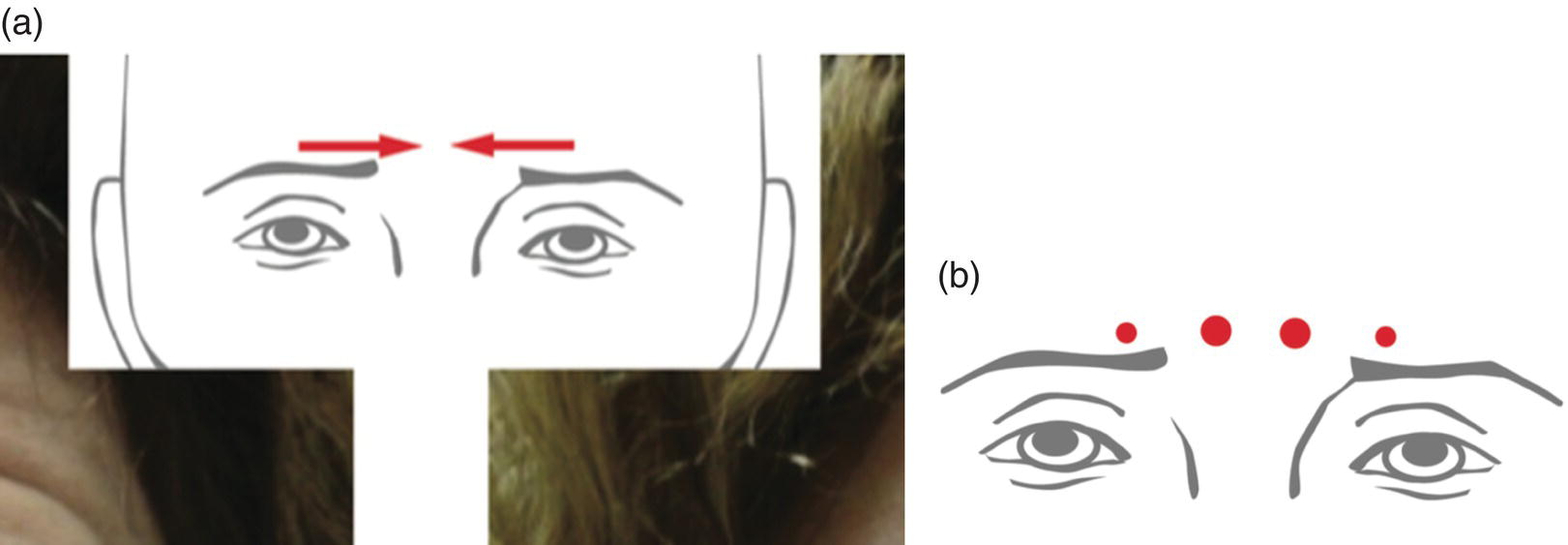
Figure 26.8 (a) Converging points pattern. (b) Injection points for converging arrows pattern.
This classification system enables a more accurate, individualized treatment with BoNT. Muscles that are more recruited, hyperkinetic, and/or hypertonic receive higher doses or more injection sites. Other less solicited muscles are injected with lower doses or not treated at all [39, 40] (Figure 26.9a,b).
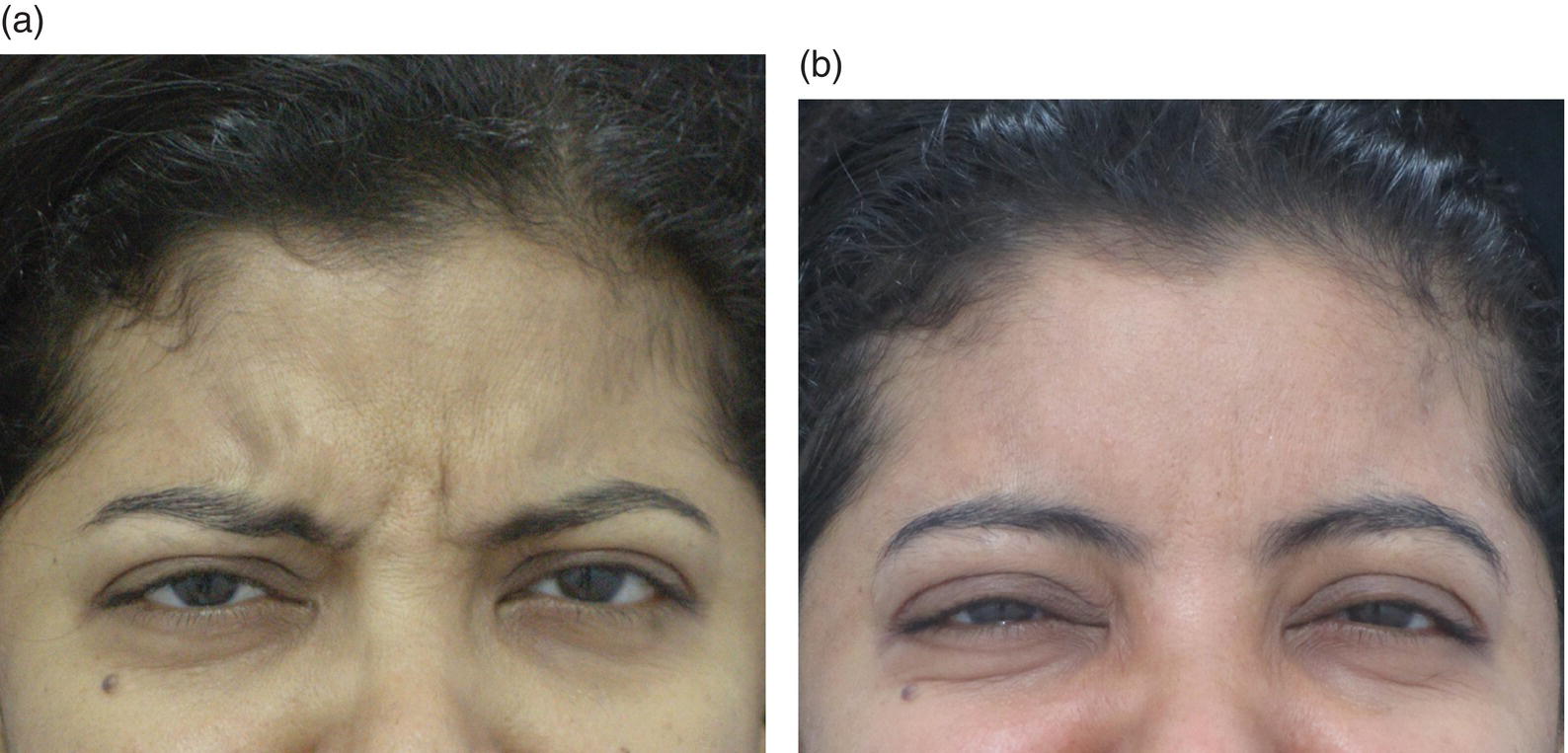
Figure 26.9 (a) Glabellar frown lines before injection. (b) Glabellar frown lines after BoNT injection.
Ethnic and Gender Differences
Asians: A more conservative approach may be warranted while treating Asian women, because of their epicanthal folds and the effects on their ability to apply makeup. Usually three injection points are sufficient to start with and a total dose of 10 units may be injected. The patient may be re‐evaluated in two weeks and more units may be injected if required [37].
Gender: The shape of the male brow tends to be horizontal. Men have larger muscle masses on average. Males tend to have thick sebaceous skin. All these factors call for higher doses of BoNT compared to females.
Complications
Eyelid ptosis occurs due to diffusion of the neurotoxin through the orbital septum into the levator palpebrae superioris muscle, which is the upper eyelid muscle. This can happen if injections are placed in the vicinity of the mid‐pupillary line, or even when one injects the lateral fibers of corrugators too close to the orbital rim with the needle pointed toward the orbital rim. It can occur as early as 48 hours or as late as 7–10 days following injection and can persist for up to 2–4 weeks. Temporary improvement of lid ptosis can be achieved with alpha‐adrenergic agonists ophthalmic eye drops apraclonidine 0.5% and phenylephrine hydrochloride 2.5%. These are mydriatic agents and cause contraction of Müller’s muscle, an adrenergic muscle, which is situated beneath the levator muscle of the upper eyelid. The treatment is symptomatic, raising the eyelid temporarily by 1–2 mm, and 1–2 drops three times a day must be continued until the ptosis resolves [41].
A higher dose in the glabella causes the medial eyebrows to appear splayed.
Tips to Get Optimum Results
- Note the type of frown lines.
- Assess the muscle mass (usually more in males).
- Study the type of brow arch.
- Assess brow position. Brow position, especially in men, may lie below the orbital margin. It is important to avoid injecting into the orbit. In women, be sure to consider whether the brows have been plucked or tattooed.
- Exercise caution in patients who have undergone surgery that can alter the underlying anatomy.
- Look for any pre‐existing ptosis or brow asymmetry.
- Always start with the minimum required doses. A touch up can be done two weeks later.
- Never inject too high above the supraorbital ridge as you may end up injecting into the lower fibers of the frontalis.
- Avoid injecting into the corrugators lateral to the mid‐pupillary line.
- Ask the patient to frown and note the dimpling as the muscle bulk ends. This is the point of insertion of the corrugators. Your last injection point should be medial to this dimpling.
- Never inject with the needle pointing toward the orbital rim. This will prevent accidental injection into the superior oblique muscle which could result in lid ptosis.
- Palpate the supraorbital rim and place the thumb finger of the noninjecting hand over the rim. Digital pressure at the border of the supraorbital ridge while injecting the corrugator also reduces the potential for extravasation of the toxin, avoiding inadvertent weakening of the levator muscle and resulting eyelid ptosis [41].
- Palpate the supraorbital notch and avoid injecting here in order to prevent pain and bruising, as the supraorbital nerve and vessels come out of this notch.
- Males may need a higher dosage compared to females due to a higher muscle mass and thicker skin.
- Soft‐tissue augmentation may be needed to treat static glabellar lines.
The Horizontal Forehead Lines
These are horizontal lines which appear on the forehead when one raises the eyebrows.
Muscle Involved
The frontalis originates on the galea aponeurotica along the coronal suture, and inserts on the dermis at the level of the supraorbital ridge of the frontal bone, where it interdigitates with fibers of procerus, corrugator supercilii, and orbicularis oculi muscles. This muscle elevates the brows. Forehead lines appear horizontally as the fibers of the frontalis are oriented vertically (Figure 26.10).
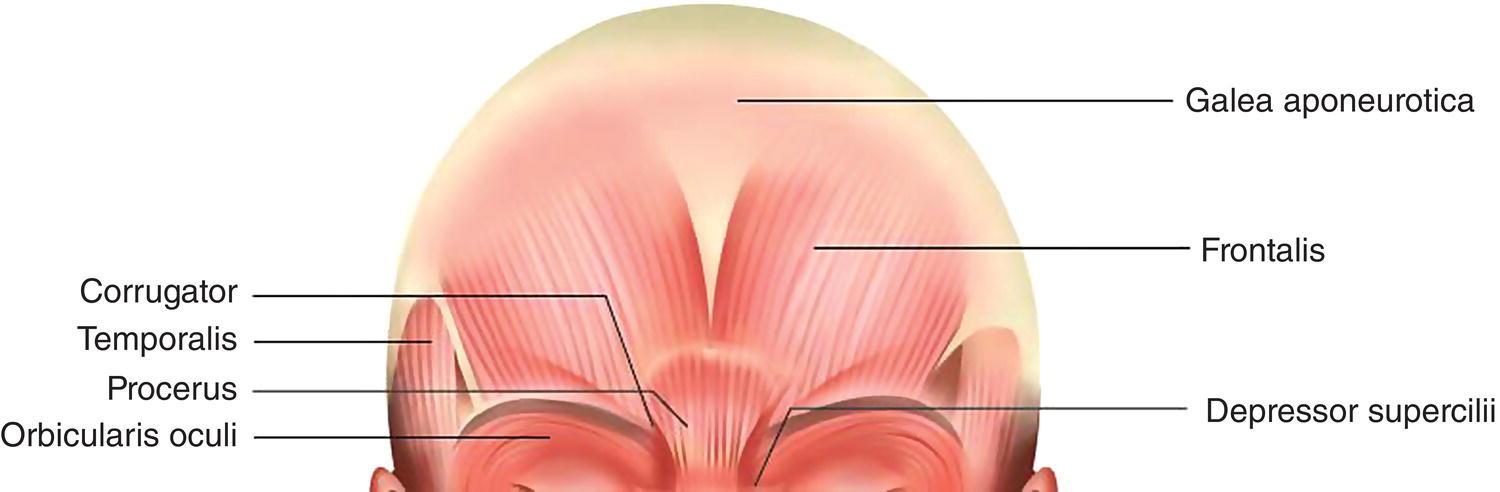
Figure 26.10 Frontalis muscle anatomy.
The key in treating the forehead is to keep a little activity of the frontalis rather than freezing it completely, as it is the only brow elevator.
Conventional Injection Technique, Sites, and Doses
In order to contract the forehead muscles, the patients are asked to elevate their eyebrows. The injection points are marked in a “Jacob’s ladder” configuration or staggered distribution, 1–2 cm apart. About one unit of the toxin is injected into each point and a total of 10–12 units may be injected in males and about 6–8 units in females depending on the muscle thickness (Figure 26.11).

Figure 26.11 Injection points for forehead lines.
Avoid injecting into the lowest fibers of frontalis i.e. in the lower third of the forehead. Stay 2 cm above the superior orbital rim in order to prevent brow ptosis.
If the patient has a low eyebrow, treatment of the forehead lines should be either avoided, or limited to the upper third of the forehead. Some patients, especially older people, use their frontalis to raise their eyebrows in order to see. You should refrain from injecting the frontalis muscle in these people. Older patients with redundant skin under the brow (pseudoptosis) should be approached with caution. In such patients, brow depressors should be treated once the brow ptosis manifests [40].
Some patients have very fine forehead lines. These people should be treated with fractional lasers or chemical peels before attempting to treat with BoNT.
Patterns
Although usually depicted as two fan‐shaped bands, the midline fibers overlap substantially in some individuals [42].
One pattern is a broad band of muscle which causes single contiguous transverse forehead lines. The second pattern shows two separate muscle bellies with a central separation. In addition, the medial fibers of the frontalis may be more fibrous than the lateral fibers [43]. Some individuals have numerous fine forehead lines, whereas others have a single deep horizontal furrow. The two muscle patterns are shown here (Figures 26.12 and 26.13), and before and after photos are seen in Figures 26.14a,b.

Figure 26.12 Two bellies of frontalis.

Figure 26.13 Single belly of frontalis.
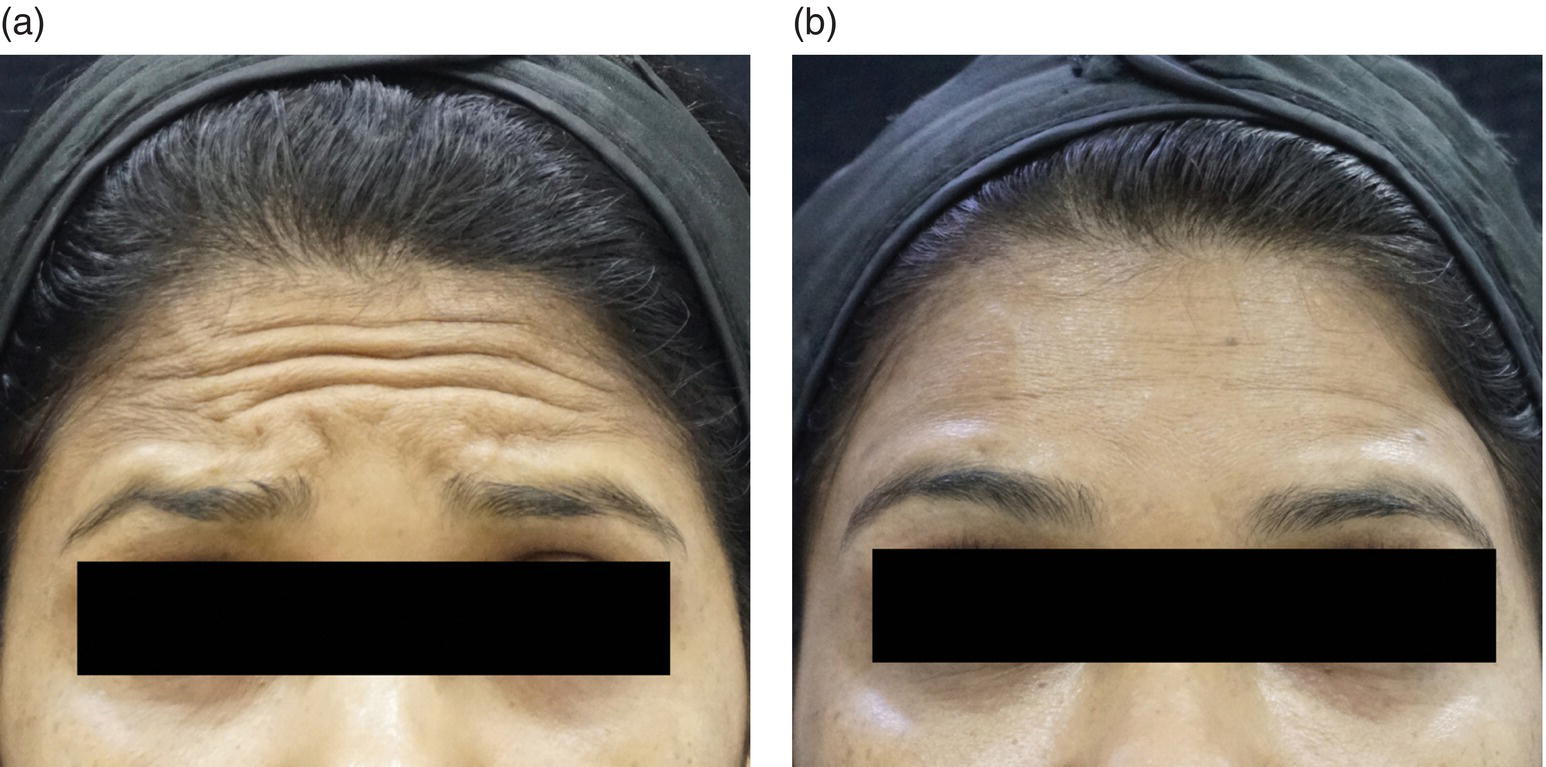
Figure 26.14 (a) Forehead lines before injection. (b) Forehead lines after injection.
Ethnic and Gender Differences
Ethnic: Asians need fewer injections for the forehead as they often have fewer wrinkles in the upper face compared to Caucasians [44]. Also, Asians tend to have the appearance of “puffy” eyelids, and any inadvertent eyebrow ptosis and heaviness of the brow will exacerbate eyelid heaviness [45].
Gender: Men have larger muscle masses on average and will require higher doses. The shape of the male brow tends to the horizontal, whereas the female brow is characterized by a gentle arch. This should be kept in mind, as injecting the frontalis can change the shape of the brow.
Complications
Brow Ptosis: Botulinum, toxin when injected within 1 cm of the bony superior orbital rim (lower portion of the frontalis), can cause brow ptosis due to unopposed action of the depressors. This can be reduced by injecting the glabellar complex. Lateral brow ptosis can be reduced by injecting two to three units of BoNT at the lateral canthus, in order to prevent the pull of the orbicularis oculi downward.
Quizzical Brow: A quizzical or Spock’s brow is seen when the lateral eyebrows arch upward to an excessive extent because of the unopposed pull of the frontalis [46]. This occurs when the lateral fibers of the frontalis muscle have either not been injected or have been underdosed compared to the medial fibers of the frontalis. This may be corrected by injecting one to two units of BoNT into the higher fibers of frontalis laterally in line with the elevated Spock’s brow (Figure 26.15).
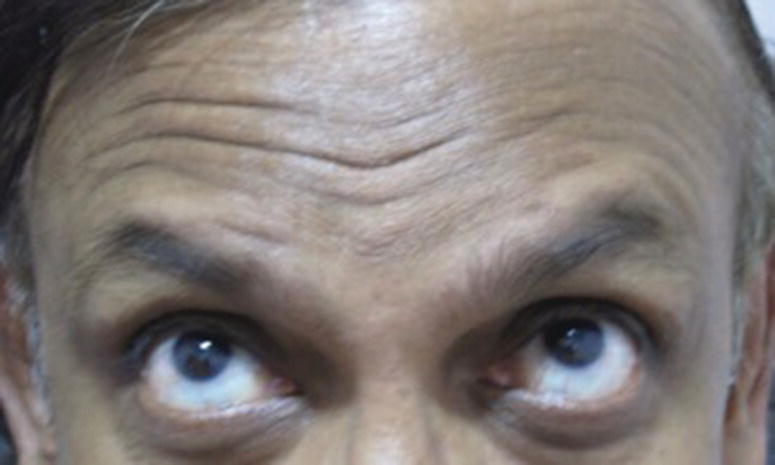
Figure 26.15 Spock’s brow.
Ptosis of the upper eyelid: Lid ptosis occurs secondarily to downward diffusion of the BoNT into the levator palpebrae superioris. This is usually a result of poor injection technique, when you inject too close to the orbital rim or point your needle toward the orbital rim. It can also occur due to overdosage of the glabellar complex and lower fibers of frontalis muscle.
Lack of expressivity or a mask like frozen face: results due to overcorrection of the frontalis muscle. Always inject low doses of BoNT into the frontalis as this is the only brow elevator.
Appearance of new wrinkles or noticeable glabellar protrusion following BoNT injection on the forehead: This was reported by Kang et al. in 2011 [47]. Hyperactivity and overcompensation of untreated muscles can cause the appearance of new lines or exaggerations of wrinkles. In people frequently using the frontalis muscle to raise their eyebrows or eyelids, exaggeration of previously unidentifiable wrinkles can take place at the border between the paralyzed frontalis muscle and non‐paralyzed frontalis muscle. Sometimes, you may see a protrusion in the glabellar area due to hyperactivation of glabellar muscles with weakness of the frontalis muscle. The only way to treat this protrusion or bulge is to inject BoNT into the glabellar complex.
Tips to Get Optimum Results
- Do not inject botulinum into the lower third of the forehead.
- In people with a small forehead, inject higher up on the forehead and keep the doses low to prevent brow ptosis.
- If the patient has a low eyebrow, treatment of the forehead lines should be avoided, or limited to the upper third of the forehead.
- The brow depressors should be treated in individuals with low‐set brows or mild brow ptosis, and probably all individuals over 50 years of age. There is upward diffusion of toxin that addresses the lower forehead lines.
- Do not leave the lateral fibers of the frontalis unopposed. This will result in Spock’s or Quizzical Brow.
- Look for brow asymmetries and correct the asymmetry.
- Distribute the injection points according to the observed animation and muscle function of the individual patient.
Crow’s feet
Muscle Involved
Lateral fibers of Orbicularis Oculi.
The orbicularis oculi muscle arises from three sites: from the nasal part of the frontal bone, from the frontal process of the maxilla, and between these two sites, from the medial palpebral ligament. The fibers then pass around the orbit in concentric loops and insert at the origin itself (Figure 26.16).
Figure 26.16 Anatomy of orbicularis oculi muscle.
The muscle comprises three parts: the orbital, palpebral, and lacrimal parts. The orbital part is the largest and extends onto the face some distance beyond the orbital rim. The orbicularis oculi muscle may be regarded as a sphincter of the eyelids. The orbital part is involved in forced closure, i.e. “screwing up” the eye. The lateral fibers of this muscle act as lateral brow depressors. As the inferior lateral orbicularis fibers curve more medially, the muscle acts as an accessory elevator of the cheek.
Conventional Injection Technique, Sites, and Doses
Ask the patient to give a big smile or to squint such that the lines become prominent. Mark one to four injection points depending on the pattern of the wrinkles, staying 1 cm lateral to the orbital rim. Keep a distance of 1 cm between two injection points. Palpate the zygomatic arch and make sure you stay above the arch. Diffusion into the zygomaticus major or minor muscles can lead to lip ptosis. Stay away from all visible blood vessels in order to prevent obvious bruising. While injecting, the needle should point away from the orbit and should be almost parallel to the skin as the muscle fibers are very superficial in this region (Figure 26.17). A tiny bleb may be raised as you inject. The recommended dose is 8–10 units per side in females and 10–12 units per side in males [48].

Figure 26.17 Injection points for crow’s feet.
Patterns
Patterns of crow’s feet lines (CFLs) vary among individuals [49].
- Type I – Full fan pattern: Wrinkles lateral to the external canthus of the eye, extending from the brow to the zygomatic arch (Figure 26.18).
- Type II – Lower fan – Wrinkles lateral to the external canthus of the eye, extending from the line of the external canthus of the eye to the zygomatic arch (absence of wrinkles in the superior lateral region) (Figure 26.19).
- Type III – Central fan: Presence of wrinkles in the line of the external canthus only (Figure 26.20).
- Type 1V – Upper fan: Wrinkles lateral to the external canthus of the eye, extending from external canthus to upper eyebrow (Figure 26.21).

Figure 26.18 Full fan pattern.

Figure 26.19 Central fan pattern.
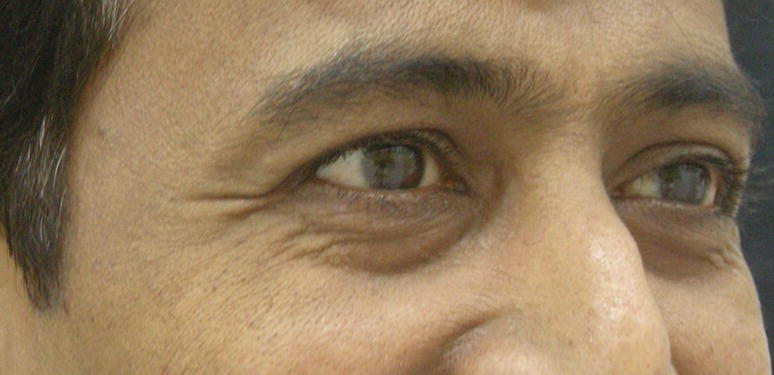
Figure 26.20 Lower fan pattern.

Figure 26.21 Upper fan pattern.
Before and after photos are seen in Figures 26.22a,b
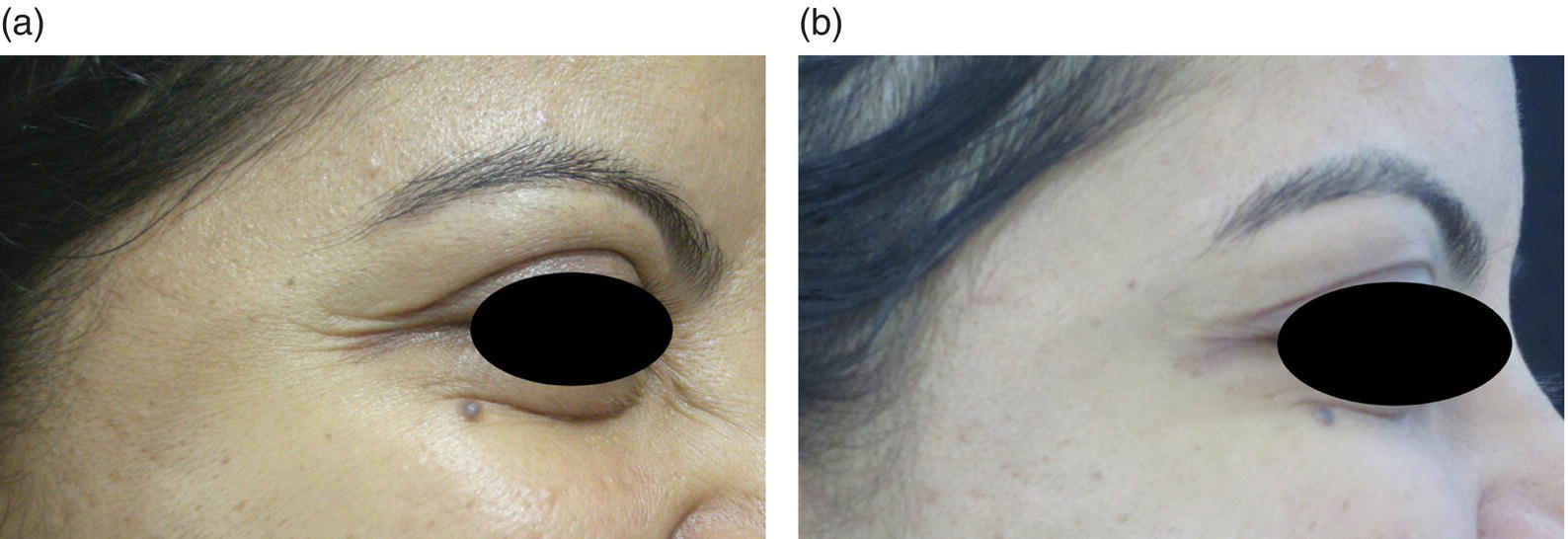
Figure 26.22 (a) Crow’s feet before BoNT injection. (b) Crow’s feet after BoNT injection.
Ethnic and Gender Differences
Ethnic: Asians have fewer wrinkles compared to Caucasians and will need a lesser number of units to treat crow’s feet.
Gender: Males usually need higher doses than females due to thicker and stronger muscles. However, males prefer to have a rustic look and usually do not prefer all the crow’s feet to be removed. Hence, always undercorrect and make the lines appear softer rather than disappear.
Complications
Asymmetric smile or Lip Ptosis: Lip ptosis can occur if the BoNT is injected below the zygoma whereby the neurotoxin diffuses into the zygomatic major and minor muscles, which are important elevators of the upper lip and mouth.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


