Botulinum toxin A is a highly efficacious and cost-effective, nonsurgical option for reducing the width and shape of the lower face and jawline. The results can vary from the subtlest thinning of the face to an extremely thin, cachectic appearance. Many nuances can be achieved. The administration is simple, and the process takes barely 5 minutes in an office setting. Botulinum toxin A can also be effectively used to reduce the bulk of an enlarged parotid gland without affecting saliva production.
Thin, waiflike models with sculpted cheekbones and fashionable hollows under these cheekbones leap out at us from every page of a glossy magazine. Female and male consumers are increasingly influenced by these images and seek facial improvements that will bring them closer to these aesthetic ideals. With these current media perceptions, in Asia, a lady with a square-shaped face and strong jawline may not be considered beautiful and can, in fact, find herself the butt of derogatory comments. There is therefore pressure to conform to the more triangular and heart-shaped classic ideal of a face.
Botulinum toxin-A (Botox) is a useful tool for the cosmetic reduction of the bulk and volume of the masseteric muscle, thereby narrowing the width of the lower face. Botulinum toxin-A can be administered in such a way as to control the degree of reduction and control whether the upper or lower half of the muscle is to be narrowed in accordance with the patient’s wishes. Consequently, the jawline becomes more well-defined and the cheekbones take on a sculpted appearance with relative, aesthetic cheek-hollowing and “model-like” shadows under the zygomatic arch.
The result is not permanent, and injections need to be repeated at least six-monthly, after an initial start-up phase in which the botulinum toxin-A is administered monthly, until the degree of desired reduction is achieved. The technique is grounded in craniofacial principles, is safe and reversible, and has few side effects. An adjunct to this technique is the concomitant administration of botulinum toxin-A to enlarged or visible parotid glands, also to achieve reduction of lower facial width and better definition of the jawline.
History
The author started this novel approach to reducing lower facial width in 1998, in response to the need for a nonsurgical and easy solution to treat patients with wide, “boxy” faces or “square jaws”. These patients complained of a masculine, aggressive appearance, lack of feminine face shape, and protruding angles of the jawline. Many patients who could not articulate the problem merely felt they looked fat in pictures. Some patients, on questioning, also suffered from headaches or migraine and some had excessive wear from grinding their teeth.
At the time, the only solution for patients with prominent mandibular angles was mandibular angle ostectomy and removal of part of the masseteric muscle (usually the inner attached portion). This was a bloody operation with significant postoperative downtime and swelling. Complications, such as nerve trauma or intraoperative fractures of the mandible, were known to happen.
Botulinum toxin-A had first been reported in 1994 as a treatment for patients with excessive grinding. As the masseter muscle was responsible for the grinding and a widened lower face, the author decided to inject this muscle to reduce its bulk and any other symptoms arising from its malfunction. This would give the patient a cosmetic and functional benefit.
In accordance with Moss’ , Rankow’s and Enlow’s theories of the bone-muscle matrix, bony growth and maintenance of volume is under the influence and related to the activity of the muscles attached to the bone. A bone responds to the activity of the attached muscles and thickens and becomes denser when there is increased muscle stimulation or when it is “force loaded”. Thus, senior citizens are encouraged to exercise to strengthen their bones and increase bone density. Conversely, in the days before rigid fixation of fractured limbs, affected bones were immobilized in plaster casts for many weeks. On removing the cast, the affected bone was always much smaller (confirmed by radiographs) than the unaffected, contralateral side, mainly because of lack of muscle activity during the immobilization period. The author also observed that patients with masseteric hypertrophy invariably had flaring of the mandibular angle and vice versa, lending further weight to the validity of Moss’, Rankow’s and Enlow’s principles. It was further reasoned that long-term changes of the bony shape could possibly be achieved if the activity of the masseter muscle could be kept to a minimum by regular and constant administration of botulinum toxin-A. Clinically, the author has seen a reduction of the protruding mandibular angle and profound changes in facial shape in many patients receiving this treatment for several years, which could not be solely due to muscle reduction.
Anatomical considerations
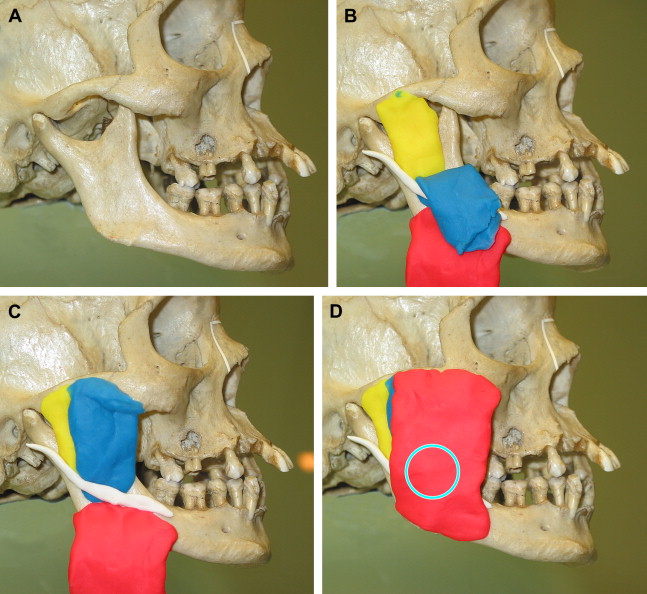
The masseter muscle arises as 3 heads from the length of the zygomatic arch, with the superficial head arising anteriorly; the intermediate head, from the middle; and the deep head, more posteriorly. The 3 heads fan downwards in reverse direction to become attached to the angle and the ascending ramus of the mandible, with the superficial head attached more posteriorly and the deep head more anteriorly ( Fig. 1 ). Thus, there is an overlap zone where the 3 heads cross each other, and this represents the thickest part of the muscle that can be palpated when patients clench their teeth. The masseteric nerve and artery run between these heads but are not at risk during the treatment because the needles used are very fine.
The limits of the muscle and hence, the botulinum toxin-A injection site are determined by palpation and observation.
The upper border of the muscle corresponds to the zygomatic arch. The posterior border is the posterior border of the mandible. The inferior border corresponds to the inferior border of the mandible, and the anterior border can be palpated when patients clench their teeth; there is a distinct difference between the soft tissues anteriorly and the masseter muscle posteriorly, which becomes rock hard on clenching.
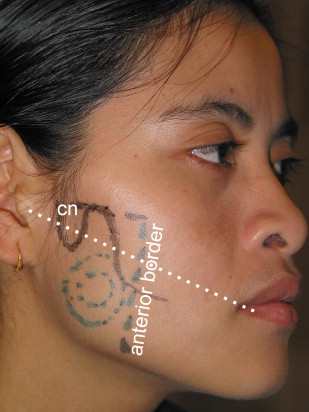
As a general guide after defining the 4 borders, a line should be drawn from the angle of the mouth to the tragus. Six to 10 injections of Botox should be administered beneath this line, to avoid unwanted diffusion through the coronoid notch to the pterygoid muscles and over-hollowing of the superior third of the muscle ( Fig. 2 ).
Anatomical considerations
The masseter muscle arises as 3 heads from the length of the zygomatic arch, with the superficial head arising anteriorly; the intermediate head, from the middle; and the deep head, more posteriorly. The 3 heads fan downwards in reverse direction to become attached to the angle and the ascending ramus of the mandible, with the superficial head attached more posteriorly and the deep head more anteriorly ( Fig. 1 ). Thus, there is an overlap zone where the 3 heads cross each other, and this represents the thickest part of the muscle that can be palpated when patients clench their teeth. The masseteric nerve and artery run between these heads but are not at risk during the treatment because the needles used are very fine.
The limits of the muscle and hence, the botulinum toxin-A injection site are determined by palpation and observation.
The upper border of the muscle corresponds to the zygomatic arch. The posterior border is the posterior border of the mandible. The inferior border corresponds to the inferior border of the mandible, and the anterior border can be palpated when patients clench their teeth; there is a distinct difference between the soft tissues anteriorly and the masseter muscle posteriorly, which becomes rock hard on clenching.
As a general guide after defining the 4 borders, a line should be drawn from the angle of the mouth to the tragus. Six to 10 injections of Botox should be administered beneath this line, to avoid unwanted diffusion through the coronoid notch to the pterygoid muscles and over-hollowing of the superior third of the muscle ( Fig. 2 ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


