Bone Reconstruction of the Knee
Robert J. Steffner
Raffi S. Avedian
DEFINITION
For this chapter, we will be discussing segmental bone loss with a specific example of a metadiaphyseal hemicortical bone defect below an intact knee joint.
Above and below the knee is a common area for segmental bone loss due to trauma, tumor, and infection.
Bone loss in the proximal tibia with an intact joint that compromises the extensor mechanism is often best reconstructed with an intercalary fresh frozen allograft with soft tissue attachments. This facilitates extensor mechanism reconstruction.
Joint loss is generally reconstructed with an allograft-prosthetic composite or endoprosthetic reconstruction.
ANATOMY
Anatomy relevant to reconstruction on the medial knee includes the adductor tendon insertion on the medial distal femur and the pes anserinus tendons inserting on the proximal tibia. The surgeon will encounter the femoral artery and vein just below the medial intermuscular septum moving through the adductor hiatus to enter the popliteal fossa.
Pay close attention to identify and preserve the saphenous nerve branch and saphenous vein.
The medial collateral ligament (MCL) connects the medial distal femur to the medial proximal tibia. The deep portion of the ligament inserts on the proximal tibia approximately 1 cm below the joint line. The superficial portion is broad and inserts on the proximal tibia 6 to 7 cm distal to the joint line.
The MCL may need to be reconstructed as part of the surgical procedure.
On the lateral knee, the iliotibial band inserts on the proximal lateral tibia at Gerdy tubercle and the bicep femoris tendon spans the knee to insert onto the fibular head. Posterior to the bicep femoris tendon lies the common peroneal nerve. The nerve divides at the anterior fibular neck into deep and superficial branches.
The lateral collateral ligament connects the lateral distal femur to the fibular head. Reconstruction may be required with bone defect management at the lateral knee.
Soft tissue loss around the proximal tibia can create a precarious situation that is at increased risk of infection. The surgeon should maintain a low threshold for soft tissue coverage with a gastrocnemius flap or free tissue transfer.
PATHOGENESIS
This technique is applicable to bone loss from bone tumor excision, bone loss from trauma such as an open fracture, and osteomyelitis requiring debridement.
NATURAL HISTORY
Management of bone defects around the knee are a challenging problem that frequently requires multidisciplinary management between general surgery, orthopedic surgery, plastic surgery, and infectious disease.
Before instituting the described procedure, the surgeon must obtain a clean bone defect with viable tissue that is free of infection.
This may require multiple surgeries focusing on debridement, antibiotic cement spacer placement, bone stabilization, soft tissue coverage, and intravenous antibiotics to prepare the area for the described definitive procedure.
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient presentation and reason for the bone defect influence the treatment approach and time interval to the definitive bone grafting procedure.
Trauma and infectious etiologies often require serial debridement and temporary stabilization with definitive stabilization and soft tissue coverage performed once a clean tissue bed is achieved.
The surgeon should assess the neurovascular status of the involved extremity. A functional limb is a candidate for limb salvage. A severely compromised limb may be better with an early amputation.
When pursuing limb salvage, the stability of the collateral ligaments should be tested by applying a varus and valgus stress to a slightly flexed knee.
The patient should be asked to extend the knee against gravity to test the competency of the extensor mechanism.
Laboratory studies depend on patient specifics and can be used to assess nutritional status, blood count recovery after chemotherapy, and inflammatory markers to assess for infection or response to antibiotics.
IMAGING
Radiographs are used to assess defect size and provide an estimate of how much bone graft will be needed (FIG 1A). Further, the surgeon can plan implant needs to provide sufficient stabilization of the involved bone.
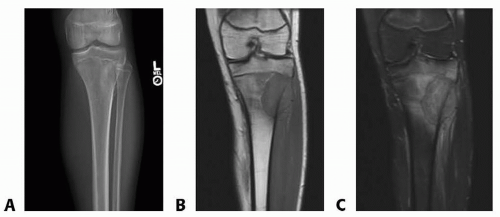
FIG 1 • A. AP radiograph, (B) coronal T1 MRI, and (C) coronal T2 MRI of a primary bone tumor of the lateral proximal tibia.
Computed tomography and magnetic resonance imaging (FIG 1B,C) provide a detailed assessment of cortical bone and offer a volumetric assessment of the defect.
SURGICAL MANAGEMENT
In the setting of a large bone defect (≥ cm), surgery is generally necessary to improve function and facilitate weight bearing. The described technique has been utilized for defects up to 2.5 cm.1
The treatment goal is to create a clean and viable tissue bed that is then filled with a cement spacer to maintain the defect space and induce formation of a biologically active, vascularized membrane (FIG 2).
After 4 to 6 weeks, the cement spacer is removed, and the defect is optimized for placement of autogenous bone grafting to facilitate reconstitution of the defect.2
The cement spacer provides structural support to the bone, offloads the implant bridging the defect, maintains the bone void, facilitates formation of the induced membrane, and can be a conduit for local antibiotic elution.
Bone graft is obtained using a reamer-irrigator-aspirator (RIA) system (Synthes, Paoli, PA).
This is a single-pass, negative pressure reaming system for obtaining intramedullary nonstructural autogenous bone graft.
Compared to the traditional iliac crest bone used for the harvest of autogenous bone graft, RIA obtains more graft volume (on average 60 cc from the femur and 40 cc from the tibia)3,4, and the graft appears to have equivalent osteoconductivity and better osteogenicity and osteoinductivity.5,6,7 Studies also suggest a greater concentration of stem cells. Harvest of bone graft with RIA is also less invasive and associated with less donor site morbidity.8
Use of RIA to obtain autogenous bone graft is indicated in skeletally mature patients with normal femur anatomy. Relative contraindications include metabolic bone disease, presence of metastatic bone cancer in the donor bone, active osteomyelitis in the donor bone, known bleeding disorder, and osteoporotic patients with thin cortices.5
Bone graft volume can be extended with cancellous allograft and demineralized bone matrix. Extension is common, and when used, we add fresh bone marrow aspirate to provide osteogenic mesenchymal stem cells to the structural allograft.6
The induced membrane is a vascularized soft tissue layer that forms around the cement spacer. It is composed of an outer layer of fibroblasts and collagen and a synovium-like inner layer. It is rich in growth factors and osteoinductive elements that include BMP-2. Upon placement of autogenous bone graft, the membrane prevents graft resorption and facilitates the formation of new cortical bone.8
Preoperative Planning
Bone reconstruction is a two-stage process.
Bone defects from infection or trauma may require serial debridement with placement of a temporary cement spacer and temporary stabilization of the bone with an external fixator or long plate. The cement spacer is often loaded with antibiotics to provide a local elution.
A clean defect can be judged by negative cultures, bleeding tissues, and maintained continuity of the defect with the intramedullary canals.
Once clean, the patient is eligible for stage 1 of this procedure.
For infection, intravenous antibiotics are generally given for the 4 to 6 weeks that the cement spacer is implanted. These antibiotics are an adjuvant and do not make up for an inadequate debridement.9
Patients are followed with serial inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) to judge eradication of the infection.
At this point, the patient has a clean bone defect that is free of infection.
The patient should be counseled on the risks of surgery, which include fracture of the donor bone, infection of the recipient site, and possible need for blood transfusion(s).
Patients should know that there may be a need to surgically stabilize the donor femur due to bone perforation by the reamer head or perceived postoperative fracture risk based on the assessment of cortical thickness after RIA use.
Patient should be aware of the donor site location and possible weight-bearing restrictions after surgery. In general, we try to use a donor bone on the ipsilateral side of the bone
defect in order to maintain one good lower extremity to aid postoperative rehabilitation.
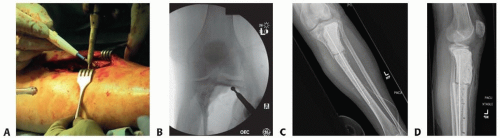
FIG 2 • A. Intraoperative preparation of the bone defect. B. Fluoroscopic view of debridement with high-speed bur. C,D. Placement of an antibiotic spacer into a proximal tibia bone defect.
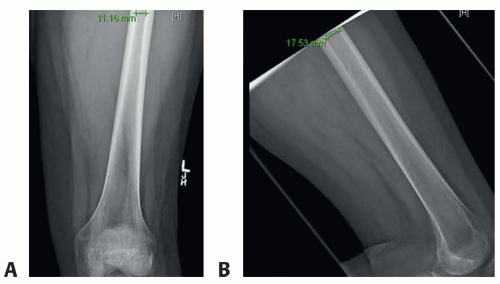
FIG 3 • A,B. Preoperative radiographs of the donor femur. The inner diameter of the isthmus is used to determine the reamer head size needed for bone graft harvest.
Preoperative radiographs are done of the donor femur (FIG 3). The surgeon assesses cortical thickness, inner cortical diameter at the isthmus, and length of the femur. This facilitates decision-making on appropriate indications for RIA use, estimation of reamer head size, and determination of the appropriate length of the RIA drive shaft (360 or 520 mm).
The size of the reamer head is determined by measuring the isthmus of the donor long bone on both AP and lateral radiographs. A head size 1 to 1.5 mm larger than the smallest measured inner cortical diameter at the isthmus should be used. If this measurement is done intraoperatively with fluoroscopy, the surgeon should factor in the distance of the ruler from the actual bone. The real canal is larger than the measurement. In general, the canal is 1 mm larger when the ruler is 2.5 cm away from bone and 2 mm larger when the ruler is 5 cm away.
To use RIA, a power driver with 3.5 to 4.5 Nm of torque and 700 to 900 rpm should be used. Drills with torque greater than 6 Nm are too powerful and should not be used.
In the operating room, the surgeon will need a radiolucent table, large fluoroscopy machine, 3-L bags of normal saline, a separate Mayo stand to hold the RIA, and a source of negative pressure suction.
A tourniquet may be used at the bone defect site if brisk bleeding is present during preparation of the area. Attempts are made to avoid tourniquet use as it can compromise the assessment of tissue viability.
The patient may benefit from a preoperative discussion with the anesthesia team regarding use of regional or neuraxial anesthesia. This can provide optimal intraoperative and postoperative pain control.
Positioning
Patient position and draping frequently requires coordination between orthopedic surgery and plastic surgery.
Position should facilitate debridement of the bone defect, harvest of bone graft, and any soft tissue coverage procedures. It may be necessary to change the patient’s position during the surgery; a repeat sterile prep and drape is then performed.
For bone defects about the knee, a supine position with a bump under the gluteus is often sufficient.
A large C-arm should be placed opposite the side where bone graft will be harvested. The monitor is positioned at the end of the operating room table.
Approach
RIA bone graft harvest from the femur is generally obtained through an antegrade approach through a greater trochanter start side. This requires an approximately 3- to 4-cm incision, approximately one hand breath above the top of the greater trochanter and 2 to 3 cm posterior to the midline axis of the greater trochanter.
Medial and lateral/anterolateral approaches to the distal femur and proximal tibia for the bone defect are well described in surgical approach textbooks.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


