Body-Contouring Procedures
Luiz S. Toledo
Lipoplasty or liposuction has changed the way aesthetic body-contouring procedures are performed. Before its evolution in the late 1970s and early 1980s, every technique involved long and permanent scars. Liposuction now allows the surgeon to reshape the body through minimal invasion. In Brazil, abdominoplasty is the procedure most commonly associated with lipoplasty: 73% of all procedures. From a historical perspective, liposuction began with descriptions of hollow cannula liposuction by Fischer in 1976.1 The technique was subsequently refined, improved, and practiced by Illouz and Fournier in the late 1970s and early 1980s.1
Body-contour treatments are frequently performed on the breasts, abdomen, thighs, and buttocks, either for reduction, augmentation, or lifting. Today, most reduction procedures of the body involve lipoplasty to some extent, with or without dermolipectomy. Augmentation can be done with autologous fat (except on the breasts) or silicone implants. Choosing the right technique is especially important when treating darker-skinned patients because of the higher possibility of hypertrophic scarring and keloid formation. However, in general, techniques are similar in all skin types and races. Body-contouring procedures are popular among blacks and Hispanics.
Classification and Contouring of the Abdomen
Although there are several classifications for the abdomen, some of which are outdated, the author prefers to classify the abdomen into six types as a template for optimal selection of lipoplasty and for abdominoplasty procedures.2 (Fig. 28-1).
A type I abdomen has excess fat, with no excess skin and no muscle aponeurotic laxity. The flanks and waist should be treated as an aesthetic unit with the abdomen when indicated. Most of these patients are treated with lipoplasty alone: either deep liposculpture for patients with good skin elasticity or superficial liposculpture (applied only in the areas where retraction is needed) for patients with skin flaccidity. Superficial liposculpture in the abdomen should be performed only by experienced surgeons. Common complications can be irregularities, skin hyperchromia, or even skin necrosis. The abdomen should be treated with the operating table hyperextended to avoid penetration of the abdominal wall.
The type II abdomen—with a high umbilicus, with moderate suprapubic excess skin, with or without excess fat, with or without muscle-aponeurotic flaccidity—can be treated with liposuction and suprapubic skin resection. The amount of skin to be resected varies from case to case. The suprapubic incision is usually a Cesarean Pfannenstiel incision with small extension into the inguinal fold.
The type III abdomen has a normally placed umbilicus, moderate excess skin in the epigastrium and hypogastrium, but not enough excess to perform a classic abdominoplasty, with or without excess fat and muscle laxity. The excess skin can be resected through a suprapubic incision and the excess fat removed through lipoplasty, thus, freeing the stalk of the umbilicus and suturing it 2 to 3 cm lower. Midline placation can be performed through the same incision, flattening the abdomen and improving the supraumbilical skin excess. If the epigastrium needs skin resection, it can be done through submammary incisions. If necessary, the epigastrium can be suctioned, without dissection, to preserve the perforators.
The type IV abdomen has muscle-aponeurotic flaccidity, excess skin, and minimum excess fat. It is treated by abdominoplasty through a suprapubic incision, skin excision, midline dissection, and muscle-aponeurotic placation, with or without umbilical repositioning. It might be necessary to close the old umbilical scar with a small vertical scar and reposition the umbilicus.
The type V abdomen has excess skin and fat in the epigastrium and hypogastrium that need muscle-aponeurotic correction. These patients should be treated with the classical abdominoplasty (Callia technique) with umbilical repositioning. The skin and fat flap from the hypogastrium are resected, and excess fat in the epigastrium and flanks is removed through lipoplasty.
The type VI abdomen with circumferential skin laxity, muscle laxity, and excess fat should be treated with a complete circumferential abdominoplasty, umbilical repositioning, and flankplasty. If dermolipectomy is continued
with lipoplasty, the dissected flap should be sutured to the aponeurosis with a quilting suture to avoid seromas.
with lipoplasty, the dissected flap should be sutured to the aponeurosis with a quilting suture to avoid seromas.
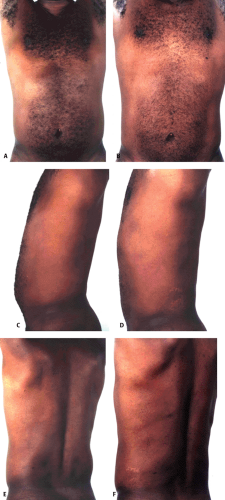 Figure 28-1 A, C, E: Preoperative photographs of a 32-year-old man wanting to improve his abdomen and flanks. B, D, F: One-year postoperative, showing improvement of the abdominal area and waist, with a 2-inch circumferential reduction after syringe liposculpture with a total removal of 1,200 cc of aspirate. |
Patients with a vertical abdominal scar are better treated using the same scar to remove excess skin combined with lipoplasty, when indicated (special type I abdomen). In the author’s opinion, the vertical skin excision in a patient with a previous scar can produce a good shape for the waist. Excess skin excision can lead to wide postoperative scars.
Thigh Contouring
There are specific treatments for different parts of the thighs. Some areas, like the lateral thighs, are more forgiving than others, and better results with simpler approaches, such as deep liposuction to remove the excess, can be obtained. Others are more difficult to treat, such as the anterior thigh and the posterior area below the gluteal fold, the so-called banana fold. These are areas that have to be treated very cautiously because of the higher possibility of provoking depressions or a “dropped buttock” look.3 The medial thigh can be a simple area to treat on a younger patient, but very difficult on an older one, with the possibility of creating skin folds that can only be fixed through a thigh lift. Usually the only area of the thighs that needs augmentation through fat grafting is the internal midthigh to correct the “cowboy leg” deformity (Fig. 28-2 and Fig. 28-3).
The thigh lift is often performed through an incision that starts in the pubic area and follows the crease of the thigh back to the gluteal fold. Skin is resected, and the subcutaneous tissue is sutured tightly to the fascia to avoid the descent of the incision below the area covered by underwear.
Buttocks Contouring
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


