Blepharoplasty: Special Considerations in the Asian Eyelid
Robert A. Goldberg
Anatomy of the Asian Eyelid and Orbit
Blepharoplasty is applied anatomy. Understanding the different surface contours of the periorbital area, understanding the bony and soft tissue substrates that create those contours, and recognizing the effects of various surgeries as they affect the surface contours are the principles of planning and executing aesthetic blepharoplasty.
No two people have identical periorbital contours. Congenital variations in bony and soft tissue anatomy and the effects of aging contribute to this variability. Even the most superficial survey of anthropology reveals obvious differences in major racial and ethnic groups with regard to periorbital anatomy. In order to successfully operate across the wide spectrum of human facial anatomy, the blepharoplasty surgeon must understand the bony and soft tissue substrates that account for variations and be able to effectively communicate with the patient to understand his/her desires and to explain the contours that can be practically changed with surgery.
The racial and ethnic variations in periorbital anatomy form a continuous spectrum, and hopefully it is obvious that there can be no cookbook approach to planning and executing surgery. There are, however, some typical differentiating features of Asian (Oriental) compared to Occidental eyelids (1, 2, 3 and 4). These differences and the surgical considerations that flow from them form a useful case study in the application of individualized decision making in blepharoplasty surgery. These differences will be the focus of this chapter. Hopefully the reader will use these considerations as a starting point for individualized anatomic analysis and individualized surgical planning of periorbital surgery across the many variations that characterize the heterogeneity of the human face.
Surface Anatomy
Static photographs fail to capture the dynamic nuances of the periorbital area. In particular, the eyebrow is a very dynamic structure. Frontalis muscle activity can
move the eyebrow 15 mm, and frontalis activity varies with emotion, attention, and compensatory drive. The eyebrow fat pad (retro-orbicularis oculi fat [ROOF]) is the most important structure in creating surface contours in the upper eyelid, more so in the Asian eyelid. The eyebrow fat pad moves in and out of the orbital space as the frontalis muscle contracts. The eyebrow position must be assessed when evaluating a patient for surgery, when determining how much loss of compensatory frontalis drive might occur after surgery, and when comparing preoperative and postoperative photographs. The ROOF fat pad is particularly full in the lateral orbit. With age, both deflation and descent of the ROOF fat occur and change the full round lateral orbit of youth into a flatter sagging structure (Fig. 4.7.1).
move the eyebrow 15 mm, and frontalis activity varies with emotion, attention, and compensatory drive. The eyebrow fat pad (retro-orbicularis oculi fat [ROOF]) is the most important structure in creating surface contours in the upper eyelid, more so in the Asian eyelid. The eyebrow fat pad moves in and out of the orbital space as the frontalis muscle contracts. The eyebrow position must be assessed when evaluating a patient for surgery, when determining how much loss of compensatory frontalis drive might occur after surgery, and when comparing preoperative and postoperative photographs. The ROOF fat pad is particularly full in the lateral orbit. With age, both deflation and descent of the ROOF fat occur and change the full round lateral orbit of youth into a flatter sagging structure (Fig. 4.7.1).
The bony orbital rim can generally not be well seen, except when loss of fat with age unmasks the contours of the deep bony structures. The orbital septal attachments to the rim can sometimes be seen in the upper eyelid and more often in the lower eyelid (although the surface contour demarcating the orbital rim in the lower eyelid more often is related to fluid bound by the orbitomalar ligament).
The superior orbital fat pads can be seen in patients who have age-related or congenital thinning of the ROOF fat (Fig. 4.7.2). A triangular hollow is present between the medial and central fat pads, related to the valley of the superior oblique and the bony notch of the superior orbital neurovascular bundle.
The eyelid crease is formed by the lowest fold of skin overlying the tarsal platform (tightly adherent skin over the tarsal plate). The epicanthal fold is a fold of skin that forms a hood over the medial canthal tendon; it probably is the single most characteristic feature differentiating the Asian (preferred to Oriental) from Occidental eyelid. The fold of skin blends variably into the upper eyelid, medial canthus, or lower eyelid. By hooding over the medial most palpebral aperture, the epicanthal fold creates a slanted appearance to the medial eyelid and a relative medial ptosis and phimosis.
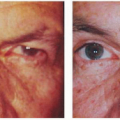
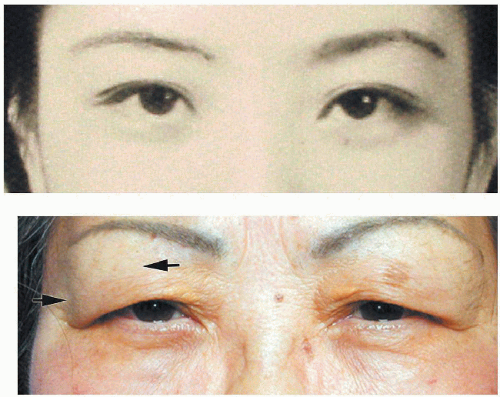 Figure 4.7.1. Patient at age 30 years and 65 years. The youthful lateral fat pad is round and full. With aging the lateral fat pad shows deflation (arrows) and descent. (Copyright 2002, Regents of the University of California, used by permission.) |
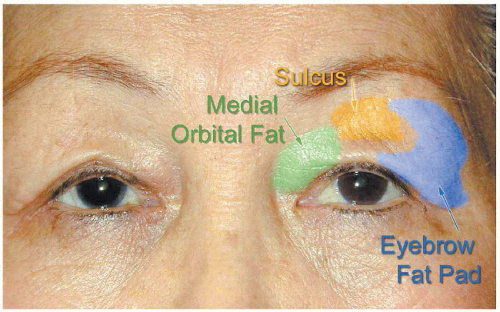 Figure 4.7.2. Aging changes in the contours of the subcutaneous fat and lateral fat pad. Note the high eyebrow position: dermatochalasis is driving frontalis compensation. The lateral eyebrow fat pad (blue) shows deflation and descent. The medial fat pad (green) becomes unveiled due to subcutaneous fat atrophy. The superior sulcus (yellow) deepens because of loss of subcutaneous and eyebrow fat, unveiling the orbital septum attachment at the orbital rim. (Copyright 2002, Regents of the University of California, used by permission.) |
Bony Anatomy
The Occidental bony orbit is angled laterally so that the lateral orbital rim is more posterior relative to the medial rim. In addition, the Occidental orbit is taller vertically; conversely, the Asian (oriental) orbit is narrower or more crowded vertically. The lateral canthus is higher relative to the medial canthus in the Asian (Oriental) orbit, 9 degrees on average compared to 5 degrees (5).
Soft Tissue Anatomy
Many authors have commented on the differences in the anatomic features of the orbital septum and orbital fat between the Asian and Caucasian eyelid (1, 2, 3 and 4). Although these differences do exist, I do not believe they are of primary importance in creating the contours that distinguish the two eyelids. Rather, I believe that the critical difference is in the subcutaneous fat and eyebrow fat pad (ROOF fat).
High-resolution sagittal magnetic resonance scans clearly point out this anatomy (Fig. 4.7.3). The eyebrow fat pad in the Asian eyelid is thicker both in the eyebrow region itself and in the eyelid space. It is this thick eyebrow fat pad that provides the full Asian upper eyelid. In addition, the thicker subcutaneous fat pad is what makes a fuller stiffer eyelid without a deep crease or with a low crease near the eyelashes. In the same way, this full subcutaneous fat pad helps to form the epicanthal fold, by filling in and stiffening the tissues medially. With age, there is loss of subcutaneous fat and loss of stiffness so that an eyelid crease forms more easily. Loss of the subcutaneous fat, and deflation of the eyebrow fat, allows a superior sulcus to form, with visibility of the junction of the orbital septum and rim (Fig. 4.7.2).
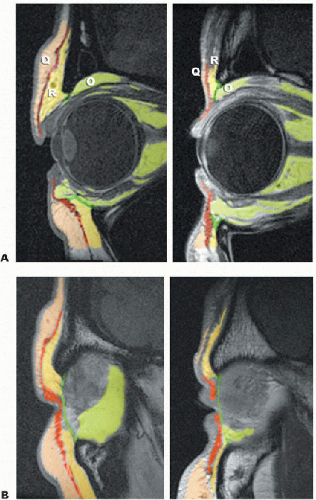 Figure 4.7.3. High-resolution sagittal magnetic resonance image. Asian orbit (A) and Western orbit (B) in young female patients. O, orbital fat; Q, subcutaneous fat; R, retro-orbicularis fat (sub-brow). The eyebrow fat pad and subcutaneous fat account for the fullness of the Asian eyelid. The vertical bony orbit is narrower in the Asian eyelid. (Copyright 2002, Regents of the University of California, used by permission. Courtesy of Joseph Demer, M.D.) |
Aging Changes
There are three general features of aging in the periorbital region. First, there is loss of elasticity of skin. This results in both static wrinkles because of loss of tone and dynamic wrinkles because of the increased ability of the orbicularis to act on the inelastic skin. Second, there is loss of volume. Deflation affects the subcutaneous fat, the eyebrow fat, and the orbital fat. Third, there is a gravitational effect on the eyebrow and cheek, as well as some gravitational effect on the globe itself, with descent and prolapse of the inferior orbital fat.
Surgical Planning
Eyebrow Fat Pad
The eyebrow fat pad is evaluated for position and volume. In youth, the eyebrow fat pad has a smooth round contour that follows the lateral orbit around. Although the Asian lateral pad is fuller, with less tendency to the curve around lateral orbit around the bony rim creating the lateral sulcus, it still has a youthful, full, smooth contour. With age, the fat pad deflates so that it has a sagging flat contour. The fat pad also descends with age so that it hangs over and hides the contours of the lateral orbit and creates redundant wrinkles in the lateral upper eyelid in the area of the orbital rim. There is no easy way to address deflation of the fat pad, but descent can be addressed with endoscopic forehead and midface lift.
Eyebrow and Upper Face
Eyebrow position is critical for blepharoplasty consideration. Every patient has some level of frontalis compensation, driven by the compensatory reflex based on eyelid margin position and eyelid skin. If we elevate the eyelid margin or debulk eyelid skin, we decrease the compensatory drive, and the eyebrow falls. This phenomenon may surprise surgeons and lead to unhappy patients who feel they look no better, or even look worse, because of the eyebrow tissues that have descended into the eyelid space. Rather, it is far better to understand the role of the eyebrow, to recognize the compensated ptotic eyebrow, and to incorporate the eyebrow into surgical planning either with upper face lift (almost always performed endoscopically) or, if this is not practical, conservative surgery designed to preserve some eyebrow compensatory drive.
Eyelid Crease and Platform
The eyelid crease is defined as the lowest fold of skin above the tarsal platform. In the Asian eyelid, there typically is only a small amount of the tarsal platform that shows, perhaps 1 to 3 mm. Sometimes, no platform shows at all. The eyelid margin position (Fig. 4.7.4), eyebrow position, lateral eyebrow fat pad, and skin and subcutaneous fat all contribute to the amount of the platform that shows. All of these factors must be taken into account when designing surgery to control the amount of the platform showing. The incision itself plays some role, particularly if there is plump subcutaneous fat and no preexisting skin fold, and the surgery is going to create a de novo fold. If the subcutaneous fat is deflated so that the skin hangs over the crease, then the incision will not actually form the crease but instead will be hidden below the overhanging skin.
Medial Canthus and Epicanthal Fold
The epicanthal fold is a critical characteristic of the Asian eyelid. It is created by complex and multicontoured anatomy of the skin and subcutaneous tissues surrounding the medial canthus and upper and lower medial eyelid. The large number of epicanthoplasties described in the literature reflects the fact that there is no simple answer to trying to alter the epicanthal fold; many of the surgeries trade a change in the epicanthal fold with a scar. Scarring can be unpredictable. I try very
hard to avoid operating on the epicanthal fold, and most of my patients accept the epicanthal fold as a beautiful part of the eyelid. Analyzing the epicanthal fold consists of determining its origin (upper eyelid, canthus, lower eyelid) and the degree of overhanging the medial palpebral angle.
hard to avoid operating on the epicanthal fold, and most of my patients accept the epicanthal fold as a beautiful part of the eyelid. Analyzing the epicanthal fold consists of determining its origin (upper eyelid, canthus, lower eyelid) and the degree of overhanging the medial palpebral angle.
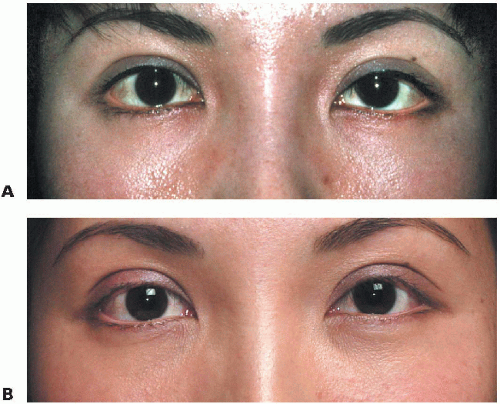 Figure 4.7.4. Eyelid margin position contributes to the height of the tarsal platform. A: Patient noted asymmetry. Blepharoplasty was recommended elsewhere. B: Only left upper eyelid ptosis surgery was performed. The change in eyelid margin position improves the symmetry of the tarsal platform and eyelid crease. (Copyright 2002, Regents of the University of California, used by permission.) |
Specific Techniques
Closed Crease Formation
In a young patient with a full eyebrow fat pad and good skin elasticity, the goal of surgery often is to alter the position of the eyelid crease. In this setting, this may be no advantage to a skin incision. In fact, closed techniques, which essentially form a full-thickness scar in the eyelid and “squeeze” the subcutaneous and orbital fat above the tight suture, have some ideal characteristics: they preserve fat, avoid the morbidity of a skin incision, and are positively perceived as minimally invasive by the patient. Although some authors have questioned the longevity of the suture techniques, my experience correlates the experience of Megumi (6) and others who report an acceptably low recurrence rate. Loss of the crease is not a disastrous complication in any case; reoperation can be used to reestablish the crease if it softens postoperatively.
Closed techniques can be used either anteriorly or posteriorly. The posterior approaches have the advantage of avoiding any visible suture or needle mark on the skin. The anterior approaches tend to provide a firmer crease, with more ability to manipulate the specific contour and position of the attachment. They do, however, involve either a suture on the skin or a small stab incision to allow the suture to fall below the skin surface (Figs. 4.7.5 and 4.7.6).
 Figure 4.7.5. Closed technique, anterior approach. Full-thickness mattress sutures are passed and tied either on the skin or allowed to fall beneath small stab incisions. A: A free needle is used to pass a 6-0 clear nylon suture from the upper edge of the tarsus out through a small stab incision at the eyelid crease. B: The suture is reloaded on the free needle, and the other end is passed from the tarsal conjunctiva out through the stab incision. C: Five sutures are passed across the eyelid. (Copyright 2002, Regents of the University of California, used by permission.) |
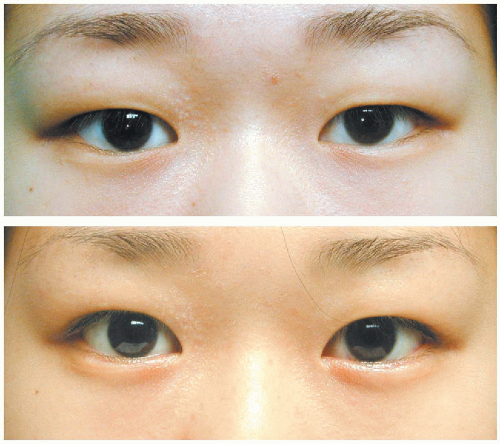 Figure 4.7.6. Anterior closed technique used to provide subtle crease elevation and rotation in young patient with eyelash ptosis and epiblepharon. Preoperative and four months postoperative. (Copyright 2002, Regents of the University of California, used by permission.) |
Open Crease Formation
Open crease formation techniques are performed through eyelid crease incision. Based on more than 50 cases, I do not believe the open technique is any more powerful than the closed technique in creating a crease. However, the open technique is used when the goal of surgery requires removal of skin, for example, in the older patient with substantial dermatochalasis, particularly if eyebrow elevation will not be performed. The technique of upper blepharoplasty is performed in standard fashion.
Some specific design considerations for the Asian eyelid are related to the crease design medially. It is best to follow the epicanthal fold toward the medial canthus and to end the incision 5 or even 10 mm lateral to the medial canthal
angle. If the incision is taken outside the epicanthal fold, there is a chance that the incision will show as a scar or that a web will develop.
angle. If the incision is taken outside the epicanthal fold, there is a chance that the incision will show as a scar or that a web will develop.
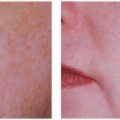
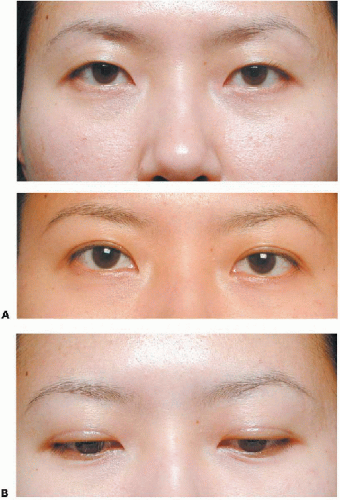 Figure 4.7.7. A, B: Open crease formation, anterior approach. Patient with no crease and full subcutaneous fat. The incision line is visible and forms a crease. The crease was drawn 5.5 mm above the eyelashes. No supratarsal fixation was performed. The crease was controlled by sculpting the subcutaneous and eyebrow fat. (Copyright 2002, Regents of the University of California, used by permission.) |
Related posts:
 Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
 Role of Chemical Peels and Other Superficial Resurfacing Procedures
Role of Chemical Peels and Other Superficial Resurfacing Procedures
 Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
 Endoscopic Brow Lift
Endoscopic Brow Lift
 Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
 Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment
Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


