15 Benign and malignant tumors of the hand
Synopsis




Introduction
• Most tumors of the hand are benign, recognized early, and treated by excision.
• Ninety-five percent of hand tumors that do not involve the skin are benign.
• Malignant tumors of the hand can be divided into two categories: primary and metastatic. Primary tumors can arise from the skin (e.g., melanoma, basal and squamous cell carcinoma), soft tissues (e.g., sarcoma), or bone (e.g., osteosarcoma). Metastatic disease originates most commonly from cancers of the breast, kidney, thyroid, lung, and colon.
• Appropriate evaluation, diagnosis, and treatment for tumors of the hand are required for optimal patient care. A careful history and physical examination will rapidly focus the investigation of a suspicious mass found in the hand.
• Magnetic resonance imaging (MRI) has become the “gold standard” to evaluate soft-tissue masses for malignancy. Computed tomography (CT) is preferred for osseous lesions.
• Incisional or excisional biopsy is required for definitive diagnosis in many cases.
• Surgical incisions must be planned carefully with definitive surgery in mind, utilizing a longitudinal incision in line with or parallel to a potential limb salvage procedure.
• Reconstructive procedures, in the setting of a neoplasm of the hand, are performed only after the final pathological diagnosis and clear resection margins are established.
• An understanding of both oncologic and reconstructive principles is required in order to achieve an optimal clinical outcome.
Basic science/disease process
Tumors of the hand can arise from the skin, adipose tissue, synovium, tendons, cartilage, bones, muscles, fibrous tissue, nerves, and blood vessels. The majority of hand tumors are benign, most are recognized early, and the prognosis is typically good.1,2 Malignant tumors also occur in the hand and can be divided into two categories: primary and metastatic. In addition, premalignant lesions such as actinic keratoses and atypical nevi can occur on the hands.
In this chapter, benign and malignant tumors are classified and discussed by their tissues of origin. Understanding the origin of hand lesions will assist in accurate diagnosis and appropriate therapeutic interventions.3
The management of hand tumors requires the hand surgeon to function as both oncologic surgeon and reconstructive surgeon. A complete understanding of both oncologic and reconstructive principles is therefore required to achieve an optimal outcome. The role of the oncologic surgeon is to eradicate the tumor completely, which can compromise both aesthetics and function. In contrast, the role of the reconstructive surgeon is to optimize hand function. Balancing these sometimes competing goals can be challenging.4
An effective strategy to evaluate, diagnose, and treat tumors of the hand and associated upper extremity is required for optimal patient care. A careful analysis of the history and physical examination will rapidly focus the investigation of a newly evident hand lesion. The use of radiography (X-rays), CT, and MRI will strengthen the apparent diagnosis.5 However, incisional or excisional biopsy will, in most instances, be the final determinant of diagnosis.
Diagnosis/patient presentation
History
A thorough history and physical examination remain the foundation of proper initial diagnosis. Questions concerning the history of the tumor are solicited. These include duration, changes in size or color, associated pain, and occurrence of ulceration. Pain can signify a malignancy or a mass that has encroached on neurologic structures. The sensitivity of the mass to cold or heat needs to be clarified, as the former typifies a subungual glomus tumor.6
The age of the patient needs to be considered when evaluating a mass in the hand. Certain masses are specific to certain age groups. For instance, bone cysts are typically seen in adolescents and young adults, whereas metastatic tumors in the hand are rare under the age of 50 years.7
Physical examination
The physical examination of the hand involves a complete examination of the skin, tendons, muscles, ligaments, bones, and neurovascular structures. An evaluation of the regional lymph nodes for adenopathy is the cornerstone for assessing the malignant potential of a hand mass. For example, adenopathy can be observed in epithelioid or clear cell sarcomas.8,9
Imaging
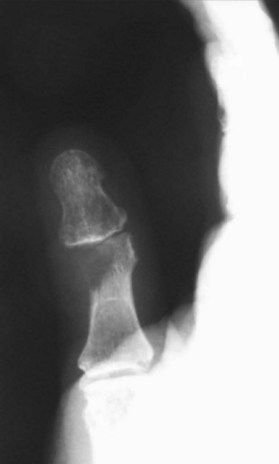
The plain X-ray is one of the most important studies for evaluating lesions and masses of the hand. X-rays are easily obtained and can evaluate a mass from multiple angles. The size of the mass can be inferred from X-rays. In the hand, a mass >3 cm in diameter should be considered potentially malignant. The architecture of the mass as it relates to the cortex of the associated bone can be determined rapidly by X-ray. Sharp cortical margins indicate a benign process, while a “moth-eaten” or destroyed cortex indicates a malignant process. Erosions and periosteal elevation on X-rays can signify a potential malignancy or an infectious process. Soft-tissue calcifications may signify a malignancy (Fig. 15.1). Rounded calcifications with central lucencies can portend a vascular etiology.
MRI is superior to CT for the evaluation of soft-tissue masses. MRI is better able to assess the intra- and extraosseous extent of soft-tissue masses. It has become the gold standard to evaluate soft-tissue masses for malignancy.10 The MRI study should include T1-weighted, fat-suppressed T2-weighted, and short tau inversion recovery images. The contrast agent gadolinium can further enhance the visualization of soft-tissue tumors. An MRI study obtained with various views can clearly delineate the extent of soft-tissue involvement prior to operative intervention. A drawback of MRI is that it cannot reliably distinguish between benign and malignant processes. In addition, for MRI of hand masses, a dedicated hand coil is required.
The next logical progression in the workup of a skin, soft-tissue, or bony lesion is a biopsy. The accuracy of pathologic assessment is dependent on the type of specimen obtained. A frozen-section analysis can be performed to assess the adequacy of the tissue sample. However, the accuracy of frozen-section diagnosis is only 80%, whereas permanent-section diagnosis is accurate 96% of the time. The accuracy of core needle biopsy is intermediate between the two, at 83–93%.2
A biopsy can be closed or open. In a closed biopsy, a needle or trephine is used to obtain samples. Closed biopsy is useful for metastatic workup. However, tissue samples from closed biopsy are often inadequate for initial diagnosis.11
Open biopsies can take many forms: the type of open biopsy performed is determined by the patient’s history, physical findings, and imaging findings. For all open biopsies, longitudinal incisions should be in line with or parallel to incisions that would be used in a later limb salvage procedure if the tumor proves to be malignant. If a tourniquet is used, the upper extremity must not be exsanguinated because doing so may cause spread of malignant cells into the lymphatics. Proper hemostasis should be maintained, and adjacent anatomic compartments should not be violated unless a radical excision is required. An important tenet is to biopsy all infections and culture all masses.3,12 Chronic infections can masquerade as malignancies, and masses can result from subclinical infections.
Enneking developed a method for musculoskeletal tumor dissection based on the histologic grade, location, and extent of the mass. An intralesional dissection is through the plane of the tumor, whereas a marginal dissection is through the tumor “reactive zone.” A wide dissection involves removal of the mass plus a margin of normal tissue but remains within a single compartment.12 A wide dissection is performed when there is a suspicion of malignancy. A radical dissection involves extracompartmental resection.
Treatment/surgical treatment by tissue of origin
Skin tumors
Neoplasms of the skin can be benign, premalignant, or malignant. In addition, there are masses such as sebaceous cysts and cutaneous horns that can masquerade as tumors but are not true neoplasms and thus are considered pseudotumors.13 For the majority of benign neoplasms or tumors, an excisional biopsy will completely eradicate the mass. For malignant skin neoplasms, such as melanoma, complete excision with clear margins does not always correlate with complete eradication of the skin tumor because of the potential for metastatic spread.1
Cutaneous horn
A cutaneous horn is an exophytic lesion that originates from the skin and is composed of keratotic material (Fig. 15.2).13 Cutaneous horns are located on sun-exposed areas of the body such as the dorsum of the hands and forearms. These unsightly lesions can interfere with function. They can occur in association with a variety of tumors, including epidermal inclusion cysts, epidermal nevi, fibromas, and pyogenic granulomas. In addition, cutaneous horns can be associated with both premalignant and malignant neoplasms such as actinic keratoses and squamous cell carcinomas. In fact, 10% of cutaneous horns are found in association with squamous cell carcinoma.

Cutaneous horns are treated by excisional biopsy with 1–2-mm margins. Incisional biopsy is not recommended for this lesion because of the potential for sampling errors.2
Epidermal inclusion cyst
Epidermal inclusion cysts are the third most common hand tumors (Fig. 15.3). These masses, which originate from an invagination of epithelium, can follow a trauma, injection, or incision.2,14 The epithelium is internalized, resulting in subcutaneous keratin deposition. Epithelial cysts are typically painless and most commonly occur in the digits.

Sebaceous cyst
A sebaceous cyst is another lesion originating from the skin and is similar in appearance to an epidermal inclusion cyst (Fig. 15.4). Sebaceous cysts arise from an obstructed apocrine gland, which produces sebum as opposed to keratin.2 When they occur in the hand, sebaceous cysts are found on the dorsal aspect. Palmar skin does not contain sebaceous glands, so sebaceous cysts do not appear there. Treatment is similar to that of an inclusion cyst, and the risk of recurrence is low.

Verruca vulgaris
The human papillomavirus causes verruca vulgaris or common warts (Fig. 15.5). Types 1–4, 7, and 10 have been implicated in the etiology of skin lesions involving keratinized epithelium. Verruca vulgaris presents as a rough raised surface anywhere on the hand and is 20 times more common than the verruca plana or flat wart, which is found commonly on the dorsum of the hand. Verrucae vulgaris are often found at sites of trauma in the periungual region (such as from habitual nail biting). The typical course of these benign neoplasms is self-limited, with spontaneous resolution in 1–2 years. However, there have been reports of malignant transformation of verrucae vulgaris, most commonly when they occur on the mucosa.15

Fig. 15.5 Verruca vulgaris. This lesion presents as a rough raised surface commonly on the dorsum of the hand.
Nevi
A melanocytic nevus or benign pigmented nevus is a benign proliferation of melanocytes (Fig. 15.6). Nevi can be either acquired or congenital. The acquired form typically begins to appear 6 months after birth, and acquired nevi increase in both number and size throughout childhood and adolescence. Congenital nevi require surveillance because of the potential for malignant transformation. Nevi are classified by size as small (<1.5 cm), medium (1.5 cm to <20 cm), and large or giant (>20 cm). The lifetime risk for malignant transformation of giant congenital nevi is 10%.16

Nevi of the hand and upper extremity should be evaluated for any clinically suspicious changes. These include asymmetry, border irregularities, color changes, diameter >6 mm, or elevation of the lesion. A useful mnemonic for these changes is “ABCDE.” When there is any doubt about diagnosis, excisional biopsy is recommended.17
Keratoacanthoma
Keratoacanthoma is thought to be derived from the epithelium of hair follicles (Fig. 15.7). This skin lesion closely resembles squamous cell carcinoma. However, keratoacanthoma growth is more rapid and central necrosis is more dominant. These lesions are typically found on hair-bearing regions. A keratoacanthoma begins as a small red papule and progresses to a large ulcerated mass. This mass is “volcano”-shaped, with a large central crater. The natural course of the lesion involves regression after a latent phase of 6 months to several years.18

Muir–Torre syndrome is an autosomal-dominant disorder associated with multiple keratoacanthomas. This clinical entity is also associated with visceral malignancy, and the workup of patients with multiple keratoacanthomas should include colonoscopy and CT.19,20
Dermatofibroma
A dermatofibroma is a fibrous tumor involving the dermis (Fig. 15.8). This neoplasm contains fibroblasts, collagen, and histiocytes. The clinical presentation is that of a firm, solitary mass of varying color. Dermatofibromas usually form in young adulthood and are found more typically in females. Excisional biopsy is performed to rule out a malignant lesion such as a sarcoma, squamous cell carcinoma, or melanoma.21

The malignant form of this lesion is a dermatofibrosarcoma protuberans, which is occasionally found in the hand.22 While the metastatic potential is low, there is a potential for recurrence after excision. A wide excision with 3-cm margins is recommended and should include underlying fascia and muscle. The likelihood of local control associated with this procedure exceeds 90%, with the probability of regional or distant metastases being less than or equal to 5%. Adjuvant radiotherapy is indicated in the event that a patient has unresectable macroscopic disease.23
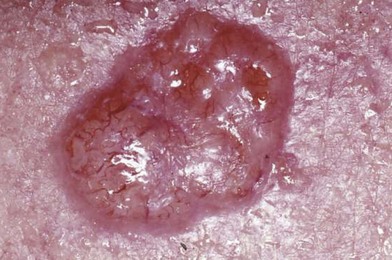
Seborrheic keratosis
A seborrheic keratosis is a benign neoplasm that originates from keratinocytes (Fig. 15.9). Seborrheic keratoses are very common, typically present in middle-aged and older patients, and can be distributed widely over the body. Initially, they appear as a hyperpigmented lesion but later coalesce into a characteristic waxy, “stuck-on” appearance. The clinical conundrum with these lesions is that, although they are benign in nature, they may mimic melanoma. These lesions require a biopsy to rule out a malignancy. If a malignancy is not suspected, these lesions can be treated with cryotherapy, curettage, or excision.

Actinic keratosis
Actinic keratoses are premalignant lesions and in fact are the most common precancerous skin condition (Fig. 15.10). An actinic keratosis presents as a rough, scaly, erythematous plaque found in an area of chronic sun exposure. The lesion is commonly tender to palpation. Histologically, this lesion shows dysplastic keratinocytes confined to the lower third of the epidermis. Actinic keratoses are the direct result of chronic sun exposure and are more common in fair-skinned persons. The potential for malignant conversion to squamous cell carcinoma ranges from 0.25% to 1.00% per year. Regression can be spontaneous if sun exposure after diagnosis is limited.

Treatment ranges from continued clinical observation to ablation. Cryotherapy can be used for isolated lesions. For more dispersed lesions, topical 5-fluorouracil, dermabrasion, and cutaneous peels such as trichloroacetic acid peel can be used. Newer reports have shown positive benefits using photodynamic therapy with porphyrin derivatives acting as a photosensitizer. Cure rates with this new modality have been reported as similar to those with topical 5-fluorouracil.24
Basal cell carcinoma
Basal cell carcinoma is the second most common skin malignancy on the hand and is the most common form of skin cancer (Fig. 15.11). Basal cell carcinomas are malignant neoplasms of the basal epithelium. Five major types of basal cell carcinoma exist: fibroepithelioma, morpheaform, nodulo-ulcerative, pigmented, and superficial. The nodulo-ulcerative is the most common form, and the morpheaform variant is the most aggressive form of the tumor. The lesions form insidiously and rarely metastasize.1,2,25
Squamous cell carcinoma
Squamous cell carcinoma is the most common malignant tumor in the hand (Fig. 15.12).26 The tumor typically presents in late middle age or later. Usually, squamous cell carcinoma is found on the dorsum of the hand secondary to chronic sun exposure. Squamous cell carcinomas are pink or skin-colored and can present as firm hyperkeratotic lesions. Since there is a potential for malignant spread, it is critical to evaluate lymph node status by physical examination.

Treatment of squamous cell carcinomas ranges from electrodesiccation and curettage for low-risk tumors to excisional biopsy for high-risk lesions. Excision with 5-mm margins of normal tissue results in complete clearance of 95% of tumors.27 Other studies have shown that wide local excision with 4-mm margins has a clearance rate of 96% and that 6-mm margins clear 99% of tumors. Metastasis is found within the first 5 years in 5% of patients with squamous cell carcinoma. This is in contrast to basal cell carcinoma, which typically does not metastasize. Long-term follow-up after treatment of these lesions is therefore critical to assess for recurrence or metastatic spread.
Melanoma
Melanoma is a highly malignant tumor of melanocytes (Fig. 15.13). Although melanomas represent only 5% of all skin cancers, they are responsible for 75% of the deaths from skin cancer.2,28 Based on these percentages, the prompt, accurate diagnosis and treatment of these tumors are critical for the well-being of all patients who present with a suspicious skin lesion on the upper extremity.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


