Axillary Surgery Versus Radiation as Treatment of Regional Nodes: AMAROS Trial and Beyond
Amanda Amin
Melissa Mitchell
History
Impact of Extensive Surgery on Clinical Outcome
Historically, breast cancer was theorized to spread contiguously through lymph nodes prior to metastatic spread. Therefore, surgical removal of the draining axillary lymphatics was recommended to prevent distant disease progression and improve survival. In the early days of breast surgery, even patients with minimal disease underwent radical mastectomy with complete axillary dissection. Ultimately, many of these patients still developed distant disease. One theory was that additional nodal disease in the internal mammary nodal chain was contributing to disease spread. Randomized studies were performed to assess the utility of an extended procedure to remove the internal mammary nodes. Results from a large multicenter trial of 1,453 patents with T1-3N0-1 disease showed no statistically significant survival benefit of extended surgical resection to include the internal mammary nodes (1). With clear evidence that comprehensive nodal surgery beyond axillary lymph node dissection (ALND) does not improve breast cancer survival, the need for axillary dissection was also brought into question.
Bernard Fisher was one of the first physicians to question whether ALND was truly therapeutic or only prognostic. He theorized that systemic control was of greater importance than extensive surgery. The first trial to assess the necessity of axillary dissection was NSABP B04 (2). On this study, 1,079 clinically node-negative women were randomized to one of three different treatment regimens: radical mastectomy, simple mastectomy with local–regional irradiation, or simple mastectomy with no irradiation. In the third arm, axillary dissection was only performed if patients became clinically positive. Local control was superior in the group that received simple mastectomy with radiation over radical mastectomy. There was no difference in overall survival (OS) between the three groups. Forty percent of patients undergoing radical mastectomy were found to have positive lymph nodes, thus 40% of patients in the simple mastectomy-alone group would be expected to have positive nodes. However, only 18% of these patients with simple mastectomy alone developed an axillary recurrence that required ALND. Only 3% of patients with simple mastectomy and radiation developed an axillary recurrence, as compared to 1% in patients who underwent ALND. There was no survival advantage for any of the three arms, suggesting that ALND could be reserved for patients who develop a clinically apparent recurrence (2).
A study by the Institute Curie performed in the era prior to sentinel lymph node biopsy (SLNB) randomized cT1-2N0 breast cancer patients to axillary dissection versus radiation to the axilla (3). All patients underwent lumpectomy followed by radiation to the breast and axilla. In the dissection group, 21% of patients were found to have metastatic lymph nodes. At 15 years, there was no significant difference between the two groups in OS (75.5% vs. 73.8%) or local recurrence (7.2% vs. 7.1%). There was increased risk of isolated axillary recurrence, though it was very low, and similar to NSABP B04 (1% vs. 3%, p = 0.04).
In the current era, systemic therapy is becoming more effective as treatments are tailored for tumor biology. Studies suggest that improved systemic therapy impacts not only distant tumor control, but also local control for breast cancer patients (4). As a result, less emphasis is being placed on the need for aggressive surgery that may cause significant long-term morbidity. This has caused a rapid pendulum shift in the surgical management of patients with locally advanced breast cancer. This chapter will review the most recent studies assessing omission of ALND for node-positive disease, with details provided in Table 29-1. It should be noted that this topic is rapidly evolving, and therefore currently accruing trials that will define the standard of care in the future for this population of patients will also be reviewed.
TABLE 29-1 Characteristics of Recent Trials of Sentinel Lymph Node Biopsy Alone in Node-Positive Breast Cancer | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Trials of Sentinel Lymph Node Biopsy Versus Axillary Dissection in Node-Positive Patients
The American College of Surgeons Oncology Group (ACOSOG) Z0011 trial is a more recent study of de-escalation of axillary surgery (5). This trial enrolled 891 patients with T1–T2 clinically node-negative breast cancer and one or two positive sentinel nodes. All patients were planned for lumpectomy and whole breast radiation. Patients were randomized to completion ALND after SLNB or SLNB alone. This study demonstrated similar 10-year OS in ALND and SLNB-alone arms (83.6% vs. 86.3%, HR 0.85, p = 0.02). There was no difference in 10-year cumulative incidence of locoregional recurrences between the two arms (6.2% for ALND, 5.3% for SLNB alone; p = 0.36). It is theorized that the incidental axillary radiation from whole breast radiotherapy may have improved local control in the axilla for patients randomized to SLNB.
Similar to the Z0011 study, the International Breast Cancer Study Group (IBCSG) 23-01 trial randomly assigned 931 patients with cT1–T2N0 breast cancer and a positive SLNB to completion ALND or SLNB alone (6). Unlike Z0011, this trial only allowed micrometastases seen on SLNB (pN1mi), making this a lower-risk population. IBCSG 23-01 allowed inclusion of patients undergoing mastectomy, though this was a small minority of the cohort (9%). IBCSG 23-01 found no significant difference in disease-free survival (DFS) or OS between the ALND and SLNB-alone groups. There was significantly less lymphedema (13% vs. 3%, p < 0.0001) and neuropathy (8% vs. 3%, p < 0.0004) in the SLNB-alone arm.
A multicenter randomized trial, AATRM, was conducted in Spain on patients with cT1-2N0 disease who were found to have micrometastatic disease at the time of SLNB (7). A total of 233 patients were randomized to ALND versus no further surgery. In patients undergoing lumpectomy, care was taken to avoid excess radiation to the axilla. As in IBCSG 23-01, only a small minority of patients underwent mastectomy (8%) and these patients did not receive postmastectomy radiation therapy (PMRT). The incidence of additional positive nonsentinel nodes was low in the ALND group (13%). There was no significant difference in local recurrence between the SLNB and ALND groups (2.5% vs. 1%, p = 0.348).
Trials of Sentinel Lymph Node Biopsy and Targeted Radiation Versus Axillary Dissection in Node-Positive Patients
The Optimal Treatment Of the Axilla-Surgery Or Radiotherapy (OTOASOR) trial was a single-center phase III study with 474 evaluable patients randomized to completion ALND versus radiation directed to the axilla (8). Patients were enrolled prior to surgery, and clinical tumor size was required to be ≤3 cm. However, patients were found to have larger tumors at surgical excision, with 21 patients having pT3 disease. There was an imbalance of tumor size in the randomized arms, with significantly more pT2 and pT3 disease in the ALND arm (57% vs. 40%, p = 0.003). In the radiation group, 60.4% of patients had macrometastatic disease. In the ALND arm, 38.5% of patients had additional positive nonsentinel nodes, and 22% were upstaged to pN2 or pN3. Only 23.3% of the ALND patients received regional nodal irradiation (RNI). All patients in the radiation arm received radiation to the level I to III axilla and supraclavicular region. Patients in the ALND arm only received radiation if they had ≥ pN2 disease or additional risk factors putting them at high risk of recurrence. With a mean follow-up of 97 months, axillary recurrence was not significantly different between the radiation and ALND arms (1.7% vs. 2%, p = 1.0). Eight-year OS was not significantly different (84.8% vs. 77.9%, p = 0.06).
The European Organization for Research and Treatment of Cancer (EORTC)’s After Mapping of the Axilla: Radiotherapy Or Surgery? (AMAROS) was a multicenter randomized trial of 1,425 cT1-T2N0 patients with a positive SLNB. As in OTOASOR, the two arms were completion ALND versus no further axillary surgery. The SLNB arm required directed radiation toward the level I and II axilla (9). Arms were better balanced than OTOASOR, with pT2 disease in 18% of patients in the ALND arm versus 21% in the SLNB arm. In the SLNB arm, 62% of patients had macrometastatic disease and 5% had ≥3 positive nodes. In the ALND group, 8% of patients were found to have ≥4 positive nonsentinel nodes. Regional radiation was delivered in the ALND group for patients with ≥4 positive nodes. As in Z0011, IBCSG 23-01, and OTOASOR, completion ALND failed to significantly impact 5-year axillary recurrence (0.43% vs. 1.19%, noninferior), 5-year DFS (86.9 vs. 82.7%, p = 0.18), or 5-year OS (93.3% vs. 92.5%, p = 0.34), when compared to the SLNB alone.
Development of breast cancer–related lymphedema (BCRL) was a secondary end point of AMAROS. The group undergoing SLNB had significantly less BCRL at all posttreatment time points. Clinical BCRL at 5 years was seen in 11% of patients randomized to SLNB and radiation, as compared to 23% of patients with ALND (p < 0.001). Objective BCRL, measured as 10% increase in arm circumference at 5 years, was 6% for the SLNB group as compared to 13% for ALND (p = 0.0009).
Z0011, AMAROS, OTOASOR, and IBCSG 23-01 have been practice changing. The 2016 American Society of Clinical Oncology (ASCO) guidelines state that ALND should not be recommended for women with cT1–T2 (≤5-cm) breast cancer who have one or two sentinel lymph node metastases and are planned for lumpectomy with adjuvant whole breast radiation therapy (10). In early-stage patients with cN1 disease undergoing
mastectomy, ALND is often recommended unless it is micrometastatic disease or there are clear indications for postmastectomy radiation, which will be discussed below. For patients with larger tumors (cT3), those undergoing neoadjuvant systemic therapy, and those with ≥2 positive sentinel nodes, axillary dissection is still routinely recommended. However, even in these higher-risk populations, the clinical benefit of surgically reducing the axillary disease burden remains a subject of debate. Multiple ongoing trials, which will be discussed below, will help to further define the population of patients who need more aggressive local therapy.
mastectomy, ALND is often recommended unless it is micrometastatic disease or there are clear indications for postmastectomy radiation, which will be discussed below. For patients with larger tumors (cT3), those undergoing neoadjuvant systemic therapy, and those with ≥2 positive sentinel nodes, axillary dissection is still routinely recommended. However, even in these higher-risk populations, the clinical benefit of surgically reducing the axillary disease burden remains a subject of debate. Multiple ongoing trials, which will be discussed below, will help to further define the population of patients who need more aggressive local therapy.
Indications for Axillary Dissection Versus Targeted Radiation to the Axilla
Surgery First
Lumpectomy patients, cT1-2N0, ≤2 nodes found on SLNB, no gross ECE: In clinically node-negative patients with T1–2 tumors undergoing upfront surgery with lumpectomy and planned for whole breast radiation, sentinel node biopsy is sufficient, as described in the previous section. The radiation oncologist should ensure that the entire level I and II axilla is encompassed in the radiation tangent portal, as shown in Figure 29-1. The decision for extended radiation to include the supraclavicular and internal mammary nodes, RNI, should be made based on careful review of patient and tumor characteristics, such as patient age, tumor size, and tumor biology, as described in the cases below.
Lumpectomy patients, cT2N0, ê 3 nodes found on SLNB or gross ECE: These patients were not included on the Z0011 trial, and only 5% of patients on AMAROS and OTOASOR had ≥3 positive sentinel nodes. As these patients were not well represented in randomized trials of SLNB alone, the standard of care is to proceed with ALND in patients with >2 positive nodes or gross ECE. These patients should receive RNI in addition to whole breast radiotherapy.
Exploratory data exists for both ALND and SLNB alone in this population. A retrospective review at Memorial Sloan Kettering Cancer Center (MSKCC) suggests that patients with gross ECE or >2 positive nodes are very high risk for additional nodal disease (11). They changed their standard practice to routinely omit ALND in
patients who met strict criteria for eligibility for Z0011. However, patients with ≥3 positive lymph nodes, gross ECE, or matted adenopathy were still recommended for completion ALND. In patients meeting these exclusion criteria and recommended for ALND, 72% had additional positive nodes. With a median follow-up of 13 months, distant metastatic disease developed in 7% of the patients recommended for ALND, highlighting the competing distant disease risk in this population of patients with more aggressive tumor biology.
patients who met strict criteria for eligibility for Z0011. However, patients with ≥3 positive lymph nodes, gross ECE, or matted adenopathy were still recommended for completion ALND. In patients meeting these exclusion criteria and recommended for ALND, 72% had additional positive nodes. With a median follow-up of 13 months, distant metastatic disease developed in 7% of the patients recommended for ALND, highlighting the competing distant disease risk in this population of patients with more aggressive tumor biology.
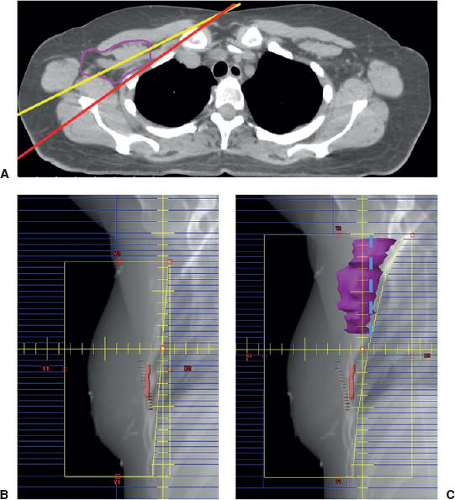 FIGURE 29-1 Radiation tangent field design for patients with a positive sentinel node not undergoing ALND. The Radiation Therapy Oncology Group breast cancer contouring atlas should be used to contour axillary levels I and II. A: A representative axial slice shows a contour of the level I and II axilla in purple, with lymphatic space contoured medial to the pectoralis minor and including the pectoralis minor. Using a standard tangent angle (yellow) may miss the posterior axilla. A steeper tangent angle (red) can improve coverage of the axilla target, while still sparing lung. B: Standard tangent fields encompass the breast alone with 1-cm superior and inferior margins on the breast tissue. C: Modified tangent fields are shown, with a raised superior border and posterior extension of the upper portion of the tangent field to include the axilla contour (shown in purple) in the radiation port. Dashed blue line depicts extension of standard tangents to the level of the humeral head “high tangent” and how a high tangent would encompass less of the axilla than 3D conformal radiation targeting this area. |
In support of omitting ALND, a SEER analysis was performed to assess outcomes for pT1–T2 patients with ≥3 positive lymph nodes found on SLNB (12). There was no difference in OS in patients undergoing completion ALND versus SLNB alone when adjusted for age, use of radiation, tumor size, hormone status, or tumor grade. As the data to support this practice is limited, omission of ALND in patients with three positive nodes or gross ECE is cautionary outside of a clinical trial, and should only be considered in the setting of low disease burden, such as low nomogram scores (13).
Lumpectomy patients, cT3N0: While OTOASOR included some T3 patients, they represented a very small portion of the population. As AMAROS and Z0011 did not include cT3 tumors, the standard of care for these patients is ALND. These patients will all require adjuvant radiation therapy to the breast and RNI.
Recommendations for ALND in this group stem from a high risk of additional nodal disease in studies of SLNB followed by completion ALND for T3 patients, in the range of 57% to 80%. Routine substitution of radiation for ALND in T3 patients should not be performed off trial until additional data is obtained. Cautious use can be considered in patients who are low risk for additional disease based on nomograms (13). All of these patients will be at high risk for distant disease, thus systemic therapy should be optimized.
Mastectomy patients, pT1–2N1mi: Z0011 excluded patients undergoing mastectomy as the primary breast surgery, and therefore this trial is not applicable to patients proceeding with mastectomy. Although both IBCSG 23-01 and AATRM included patients proceeding with mastectomy, this population was a small minority of the entire cohort (9%). Furthermore, only pN1mi patients were included (6,7). Patients with pN0(i+) or pN1mi disease may be considered for SLNB alone, even if PMRT is not planned, in the setting of biologically favorable disease. Patients with highly unfavorable features, such as young age, unfavorable tumor biology, large primary tumor, should be treated similar to patients with macrometastatic disease (pN1).
Further data to support this practice includes a retrospective study from MSKCC that reviewed outcomes of node-positive patients undergoing mastectomy and SLNB alone, no radiation (14). The majority of mastectomy patients in this study had isolated tumor cells (ITCs) at SLNB (54%, pN0[i+]) and 37% had pN1mi disease. Only 9% had pN1 macrometastatic disease. Almost all of the patients (99%) were pT1–2. Patients included in this study had low risk of additional axillary nodal involvement, with a median risk of nonsentinel axillary nodal metastasis of 9% per the MSKCC nomogram. None of the patients with pN0(i+) disease developed an axillary recurrence. Excluding those with ITCs, the 4-year local and regional recurrence rates in this study were very low for node-positive mastectomy patients with pN1mi and pN1 disease (1.2% and 2.5%, respectively).
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
 Optimizing Mastectomy Flaps Based on Breast Anatomy
Optimizing Mastectomy Flaps Based on Breast Anatomy
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


