Facial volume loss is an important component of facial aging, especially in the periocular region. The authors evaluate the normal and aging anatomy of the periocular region and then discuss volume restoration of this region using hyaluronic acid, calcium hydroxylapatite, and autologous fat transfer. Preoperative assessment, operative technique, postoperative care, and complications are addressed.
Volume loss has increasingly been recognized as an important aspect of facial aging. This is especially true of the periocular region. Restoration of this lost volume can be achieved through placement of syringe-based fillers, autologous fat, or implants. This article discusses the use of syringe-based fillers (hyaluronic acid, calcium hydroxylapatite) and autologous fat to rejuvenate the periorbital region.
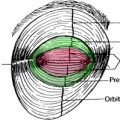
The periorbital complex consists of the brow, superior orbital rim, upper eyelid, lateral canthus, lower eyelid, inferior orbital rim, and upper cheek. The most important of these in the aging process of volume loss is the interface between the lower eyelid and upper cheek or midface. Systematic aging begins throughout the periorbital complex beginning in the patient’s mid-to-late 30s. The extent and rapidity of periorbital aging varies between individuals and is strongly dependent on the relationships between the bony orbit, globe, and malar complex. The periorbital area ages at a faster pace and earlier in life with a negative vector midface, much as the jaw line and neck age earlier in people with microgenia and a short thyromental distance ( Fig. 1 ). Some individuals even display “lower eyelid bags” in youth; these bags appear early because of the negative vector produced by the deficient anterior projection of the inferior orbital rim in relation to the globe.

Youth
The youthful upper periorbital complex consists of a brow that is full over its entire height, being propped up by the volume of the brow fat pad. Entire articles have been written and rewritten about the normal aesthetic height of the brow. The authors are well aware of these aesthetic norms but maintain that patients differ tremendously regarding their natural brow height. They ask their patients routinely about their brow position in youth and strive to restore this relationship, only changing natural brow position after careful consideration. Comparing photos in the latest fashion magazine shows many examples of models, all of whom are exquisitely attractive, with significantly differing relationships between the brow and superior orbital rim ( Fig. 2 ). The upper eyelid also shows a variable fullness between patients; all may be considered youthful and attractive. Some individuals have significant tarsal show with a deep superior orbital sulcus, a high lid crease, and very little dermatochalasia. Others have very little tarsal show with a more prominent orbital fat component and therefore, a much fuller-appearing upper eyelid and a tendency toward greater dermatochalasia. In the authors’ opinion, the restoration of the youthful upper eyelid and brow complex must be tailored to each patient’s unique characteristics and must strive toward the restoration of youthfulness and not an ideal appearance based on the biases of the surgeon. Some rejuvenation of the upper eyelid complex relies on surgical lifting procedures that are beyond the scope of this article. However, restoration of the upper periorbital volume is addressed.