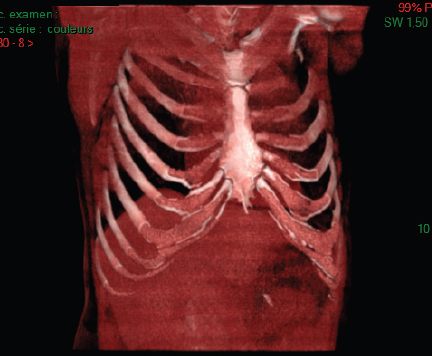
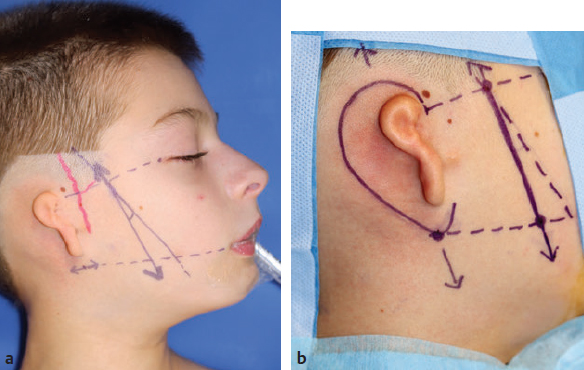
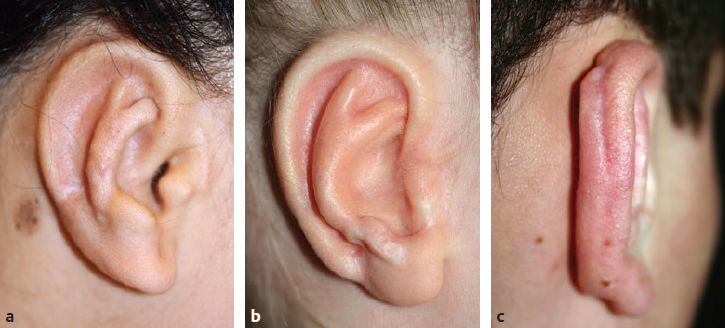
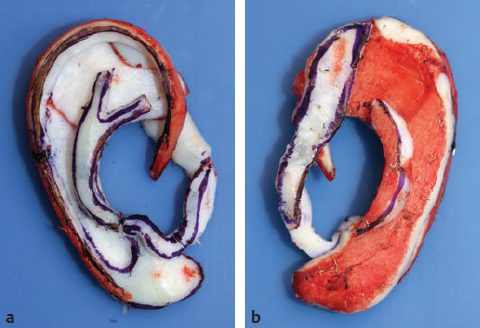
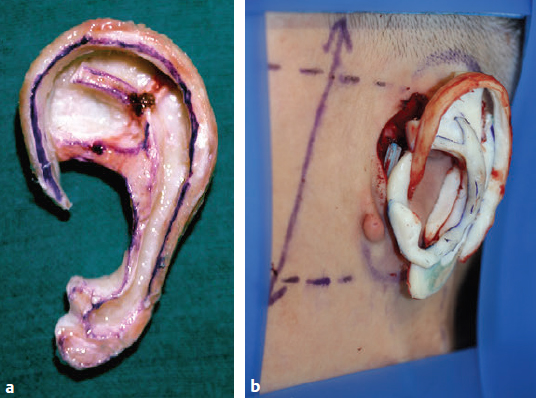
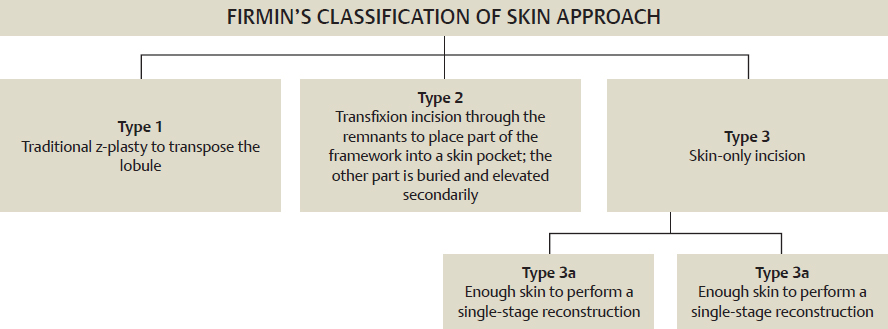
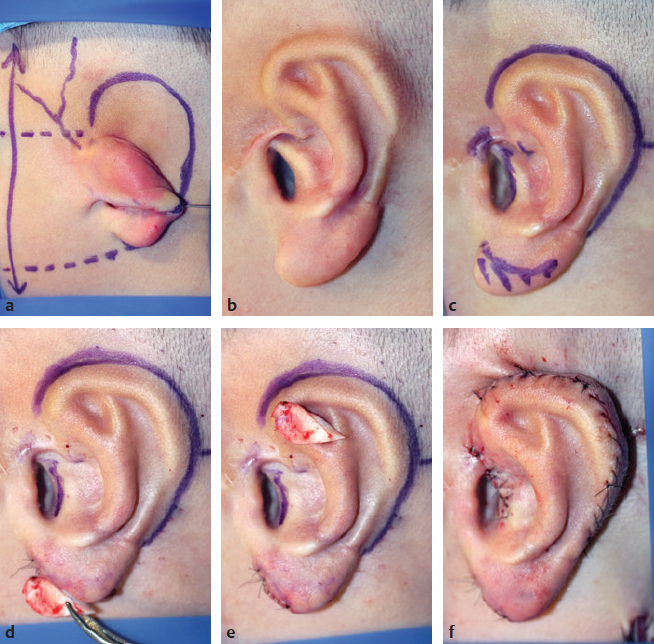
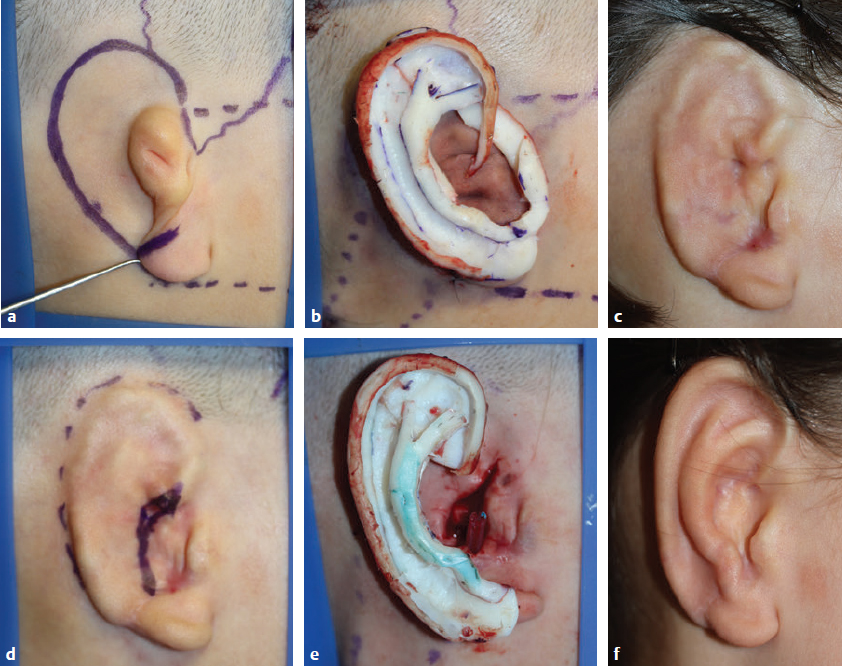
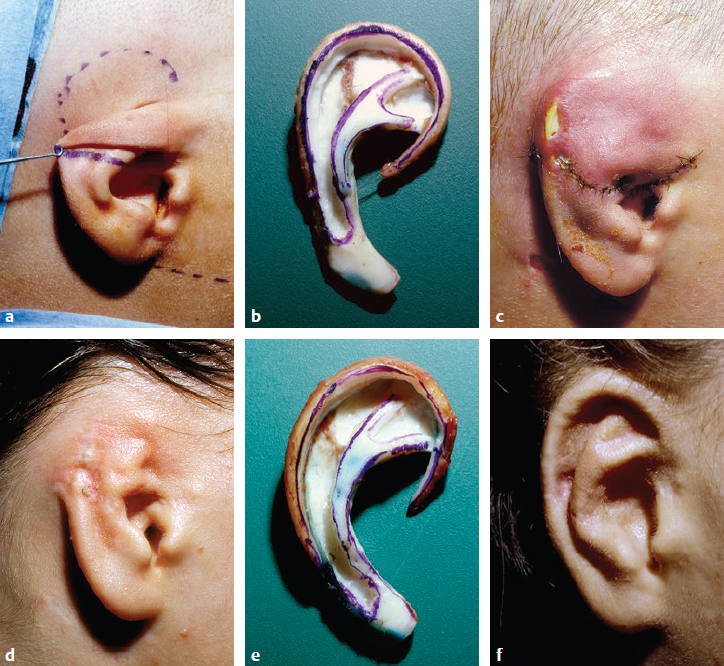
CHAPTER Neither myself nor anyone else has anything to learn from success, but only from failures and complications … Success always leads to self-satisfaction and therefore not to improvement … We should live in a world of complications … and have the courage to investigate the causes that are not always flattering: poor indications, disorganization, ignorance and haste. —The World of Complications Translation of a text written by Dr. Paul Tessier Auricular reconstruction can probably claim the award for the longest learning curve in plastic surgery, and surgeons who simply “give it a try” usually end up with very unsatisfactory results. Indeed, it takes time to learn how to sculpt a harmonious framework from costal cartilage, and, despite a sound knowledge of flaps, probably just as much to learn how to safely cover it with a thin layer of skin. Until three-dimensional printing of bioengineered frameworks becomes a reality, an ear still has to be reconstructed using a support from autologous rib cartilage or synthetic material. We strongly prefer to use costal cartilage for its ability to be precisely shaped into the form of the contralateral ear, its resistance in case of exposure, and its longevity. Over three decades, I (F.F.) have reconstructed more than 2,400 ears1,2 and have systematically applied the principles of my mentor, Paul Tessier, to critically analyze complications, to treat them, and to try to avoid them. The goal of this chapter is to highlight the hurdles along the path of ear reconstruction and to provide guidelines to avoid them. Summary Box The Most Common Problems Related to Ear Reconstruction • Skin necrosis (the most common complication) • Inaccurate design of the framework • Poor projection of the framework • Malposition of the framework • Infection (the most severe complication, because it induces resorption of the cartilage) Patients referred for an ear reconstruction can be sorted in two very different categories: 1. Children with a congenital anomaly who have never had an operation. 2. Posttraumatic cases, mostly in adults. The presence of scars stresses how the analysis of the skin potential is essential. Planning the cartilage skin coverage is the most challenging part of an ear reconstruction, and incorrect planning is the most common source of unfavorable results and complications. Each case is different, but understanding the different possible skin approaches makes it possible to select the most appropriate one for each case. Evaluating the expectations of an adult patient or those of a child’s parents is important, particularly when local conditions are not ideal. During the first consultation, and after drawing the contours of the ear on a template and placing it on the ideal position, the surgical planning (contours to reproduce and skin approach to use) is established. It is essential to draw the contours of the nondeformed ear to determine those that must be removed from the deformed ear and those that must be reproduced when carving the cartilaginous framework. This analysis will also predict the amount of cartilage needed. Preoperative planning includes computed tomography of the thorax and three-dimensional maximum intensity projection (MIP) reconstruction of the ribs to recognize ossifications of the cartilage, which will dictate which ribs to harvest (Fig. 44.1). Learning to correctly place the reconstructed ear is essential and relies on selecting landmarks from the normal side, which are drawn and used on the affected side. We commonly see patients for a secondary reconstruction in whom the axis of the ear has been placed too vertical, the ear too anterior and too low. To avoid malposition of the newly reconstructed ear, landmarks are drawn on the auricular area: • Axis of the nasal dorsum and axis of the normal ear • Level of the lobule and of the root of the helix • Distance from the lobule to the corner of the mouth, and distance for the root of the helix and lateral canthus • Contours of the framework During the skin preparation with povidone iodine, these landmarks tend to fade, and we recommend incising the key points with a 25-gauge needle. The course of the superficial temporal artery is marked using a handheld short-depth Doppler probe. Ectopic courses are common in syndromic microtia. The superficial temporal fascial flap is the workhorse of secondary reconstructions and must be preserved at all cost (Fig. 44.2). The shape of the framework is directly seen under the thin skin covering it, and the quality of the result is directly dependent on the harmonious contours of this framework. Several typical mistakes must be avoided when sculpting the framework (Fig. 44.3): Fig. 44.1 Computed tomography of the thorax and three-dimensional maximum intensity projection reconstruction of the ribs to discover ossifications of the cartilage, which will dictate which ribs to harvest. In this case, the right eighth rib is less ossified than the left one and will make a better helix. Fig. 44.2 (a) Landmarks are drawn to avoid malposition of the new ear: (1) axis of the normal ear relative to the nasal dorsum; (2) level of the lobule and of the root of the helix; (3) distance from the lobule to the corner of the mouth, and distance for the root of the helix and lateral canthus. The course of the superficial temporal artery is marked using Doppler mapping. Ectopic courses occur in syndromic microtia framework. (b) Contours of the framework are drawn in the ideal position. Because a limited operating field is prepared to avoid infection from nasal or oral cavities, it is essential to keep all these landmarks until the end when placing the framework. Fig. 44.3 Typical mistakes can be found in the design of the framework. (a) The concha is too small. (b) The posterior root of the antihelix is too prominent. (c) The posterior edge of the framework is too thick. • The concha should not be too small. • The posterior root of the antihelix should not be too prominent. • The posterior edge of the framework must not be too thick. A small concha is a very common mistake. A harmonious ear has a large concha and a very narrow groove between the helix and the antihelix. The antihelix has two very different roots. The anterior one is sharp, whereas the posterior one has a smooth curve which blends into the scapha. We have begun to carve our posterior root much smoother. Because the framework is made of costal cartilage, it is much thicker than an original ear, made out of “fibrocartilage” (which is actually elastic cartilage). The posterior edge must be thinned before implantation; otherwise the framework will be very bulky after the second stage when seen from behind. Taking these mistakes, which became evident when following our patients and critically observing our results, into account, we began to carve our framework differently (Fig. 44.4). Fig. 44.4 Our current typical complete framework. (a) The framework includes a base, a helix, an antihelix, a tragus–antitragus, a projection piece (P1), and a projection piece (P2). (b) A segment of cartilage is kept under the thoracic skin for the second stage. Note the wide concha with a very narrow groove between the helix and the antihelix, the smooth edge of the posterior root of the antihelix, and the thinned posterior edge of the base. Evolution in carving is evident when comparing a frame work carved as a beginner 30 years ago and a recent one (Fig. 44.5). The worst complication in ear reconstruction is infection, although it is not common. In our experience, infection occurs when there is an unclean external auditory canal, and the bacteria is usually Pseudomonas aeruginosa. To prevent infection, patients with an external auditory canal are systematically sent for a preoperative cleaning under microscope, and we prescribe daily ciprofloxacin droplets in the ear for 5 days before the surgery. The most common complication is skin necrosis. When performing the first dressing change on day 3 after surgery, the skin blood supply is appreciated. If the surgeon has any doubt regarding vascularity, he or she must wait until at least the eighth postoperative day to clinically confirm the presence of skin necrosis. Rib cartilage is resistant to exposure and can stay exposed for several days, covered by a moist dressing with petroleum jelly and fucidic acid. When the exposure affects a small area in a hollow (i.e., the concha, the scapha, or the intertragal notch), it should be left to heal secondarily, because it will not be visible if the cartilage resorbs. Nevertheless, when it affects a hill (i.e., the helix, antihelix, or antitragus), it should be covered by a skin flap or a fascial flap to prevent cartilage resorption. Careful planning of the skin incision decreases the risk for skin necrosis. We follow the principles outlined in our classification of skin incisions3 (Fig. 44.6). Fig. 44.5 (a) This framework was one of our first. It was made out of two pieces, a base and a helix. Retrospectively, it has little to no projection, and the result was very disappointing. (b) Now our typical framework has many hills and valleys, with multiple pieces and extra projection. Besides adding the antihelix in the anterior surface of the base, we routinely add projections behind the base. Good three-dimensional reproduction of the contours and correct positioning of the framework are evident. Fig. 44.6 The classification of skin approach. Choosing the type of skin approach depends on the remnants. Type 1 is the traditional z-plasty described by Burt Brent4 and modified by Satoru Nagata,5 which we no longer use. We prefer type 2 or type 3, which have less risk of skin necrosis. Fig. 44.7 (a) Conchal-type microtia. A type 2 skin approach is performed. (b) A critical analysis of the result after the first stage showed that the ear was a little bigger than the other (not shown), that the meatus was too visible, the concha had too sharp an anterior border, and the root of the helix was lacking projection. When performing the reconstruction of the retroauricular sulcus (c), a direct approach of the inferior extremity of the framework (d) makes possible its reduction (e). (f) This little piece of cartilage will be placed in a tunnel behind the root of the helix to improve the projection of the upper part of the ear at the end of the second stage, after skin grafting to reconstruct the sulcus. When a surgeon becomes an expert, patients are referred to the surgeon from far away. Nonetheless, the follow-up is essential after both stages, and patients must be followed by the operating surgeon for at least 2 weeks. At the follow-up several months after the first stage, a critical analysis of the result is critical before planning the second stage. Some revision of the contours may be determined necessary; this can be performed when elevating the ear (Fig. 44.7). If the contours are deceiving because of a resorption of the cartilage, generally because of an infection that may have occurred secondarily after a trauma or extrusion of wire sutures or another cause and was not efficiently cured, it is essential to start the reconstruction from scratch and to help the patient to accept this solution, even if the patient must travel far for the second stage (Fig. 44.8). Fig. 44.8 (a) This patient with lobular-type microtia presented with good skin quality. (b) When the patient left to go back to his home country, which was far away, a very good result was expected. (c) Two months later, a picture was sent by the patient that showed an inflammatory process. Antibiotics were prescribed by a local doctor, and the inflammatory process disappeared. (d) However, when the patient was seen by the surgeon 6 months later, loss of contours was evident and a new reconstruction was elected. (e) Cartilage was harvested from the other thoracic side for the new framework. (f) There was great improvement when the patient returned 6 months later for the second stage. When an infection occurs, samples are taken to bacteriology and appropriate oral antibiotics are prescribed. Antibiotics diffuse poorly in the cartilage, and bacteriologists typically recommend high doses of intravenous (IV) antibiotics over the span of 2 weeks. Unfortunately, we have not found this to make any difference in terms of cartilage resorption. Therefore we do not recommend hospitalizing patients for prolonged administration of IV antibiotics. Daily dressing changes with topical treatment are performed, and the patient is seen once or twice a week in the office. The patient and family should be told that once the infection resolves, the site must be monitored for resorption and a complementary stage may be indicated. We wait at least 6 months to perform this complementary stage. All signs of inflammation must have subsided, and the remaining contours should be stable. A new reconstruction may be indicated (Fig. 44.9). Fig. 44.9 (a) Conchal-type microtia with good skin quality. (b) The framework does not include the tragus and antitragus, which are present surrounding the auditory canal. (c) One week after the reconstruction, infection is evident, evidently coming from the canal. Pseudomonas aeruginosa was the infecting agent. (d) Intensive local and general treatment did not prevent resorption of the cartilage. (e) One year later, a new costal cartilage framework was sculpted from the contralateral side of the thorax. (f) Five years later, the patient is happy with the result despite an extrusion of wire suture on the antihelix, which can be easily removed. Primary infection has never occurred in a patient without an auditory canal; thus our assumption is that infecting agents come from the auditory canal. As mentioned previously, preoperative cleaning is essential. An autologous rib cartilage framework is a three-dimensional structure placed under the thin skin of the auricular area. Two very important factors must be considered: 1. The skin potential needed to avoid excessive tension on the skin 2. The skin approaches used to insert the framework and to avoid poorly vascularized flaps As mentioned, when skin necrosis occurs, it usually causes cartilage exposure. Skin flaps from the auricular area are rarely usable to cover the defect, but around the ear are multiple fascia layers that can be used with an axial vascularization (e.g., the superficial temporal artery, the posterior auricular artery, or the occipital artery),6 or random fascial flaps can be used (Fig. 44.10).
44
Auricular Reconstruction
Avoiding Unfavorable Results and Complications in Auricular Reconstruction
Preoperative Planning and Patient Selection
Contours to Reproduce
Preoperative Drawings
Intraoperative Considerations
Avoiding Postoperative Complications
Infection
Skin Necrosis
Managing Unfavorable Results and Complications in Auricular Reconstruction
Personal Unfavorable Result
Infection
Skin Necrosis
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine










