Augmentation mastopexy is generally considered to be one of the most difficult operations in breast surgery. It has an undeserved reputation for high complication rates and unhappy patients. Through careful planning, surgical techniques involving manipulation of the breast while maintaining blood supply and implant cover, and good augmentation technique, the operation can achieve predictable results in most cases with a low complication rate. Techniques to assess and manage the 2 main complications of waterfall deformity and bottoming out are discussed.
Key points
- •
Augmentation mastopexy is safe and predictable to perform in 1 stage in most patients.
- •
Technique is aimed at performing a good augmentation and performing the lift using breast modification while protecting blood supply.
- •
The 2 most common complications may be managed in a logical predictable way by identifying and preventing the primary cause.
Augmentation mastopexy is generally considered to be one of the most difficult operations in breast surgery. Over the years, this has resulted in advice to avoid attempting the operation in one stage because of the assertion that it was prone to a high complication rate and associated with a high risk of patient dissatisfaction. There are numerous articles attempting to improve the quality of outcomes from this difficult operation. Large series from well credentialled authors have shown that it can be performed with an acceptable complication rate. As such, the ability to select appropriate cases and plan and perform the procedure should be part of the armamentarium of all plastic surgeons performing breast surgery.
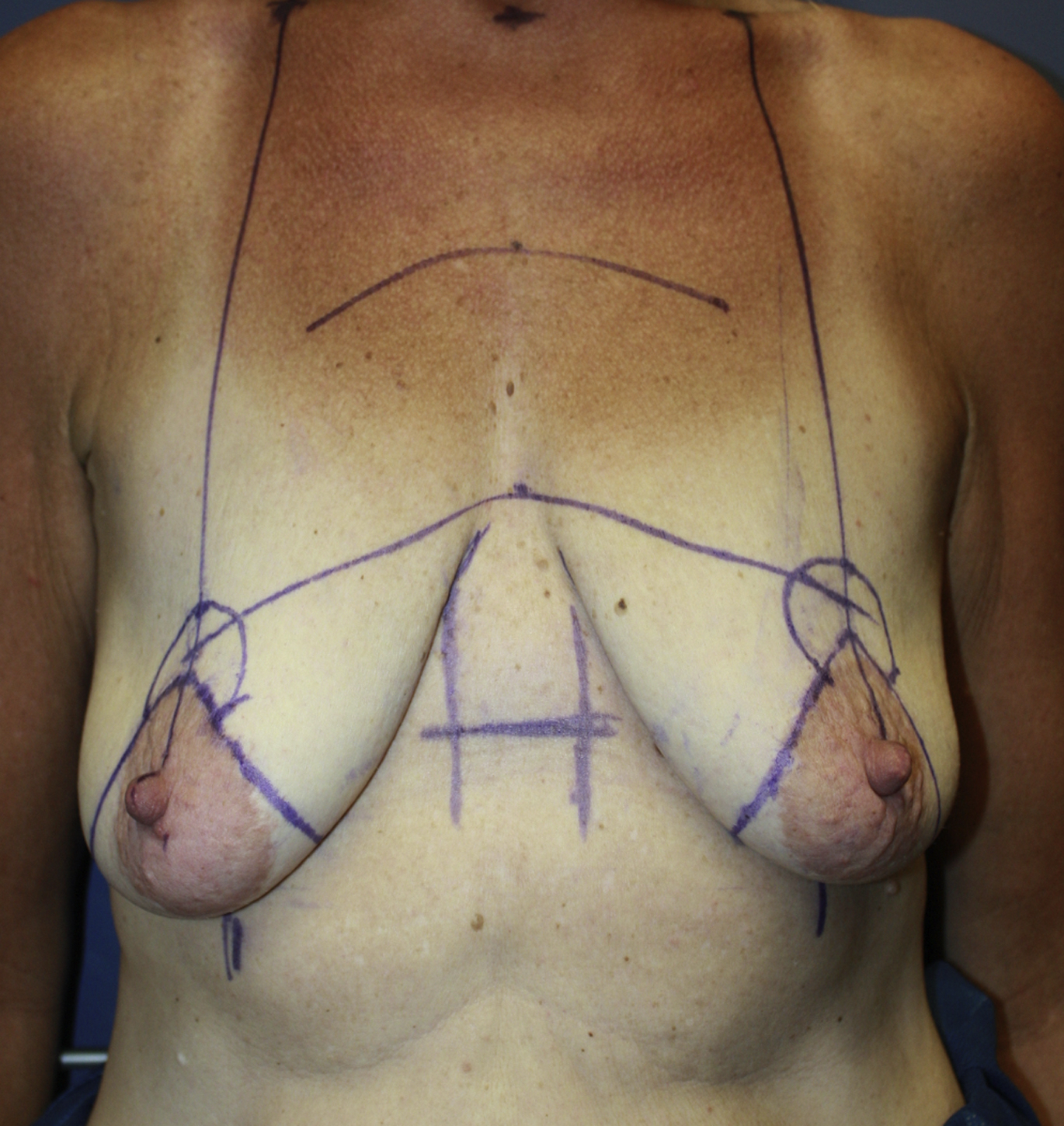
The conditions requiring augmentation mastopexy are varied and include juvenile ptosis, congenital or acquired asymmetry, postpregnancy and breastfeeding, and breast atrophy, whilst cases related to massive weight loss after bariatric surgery are increasing ( Fig. 1 ).
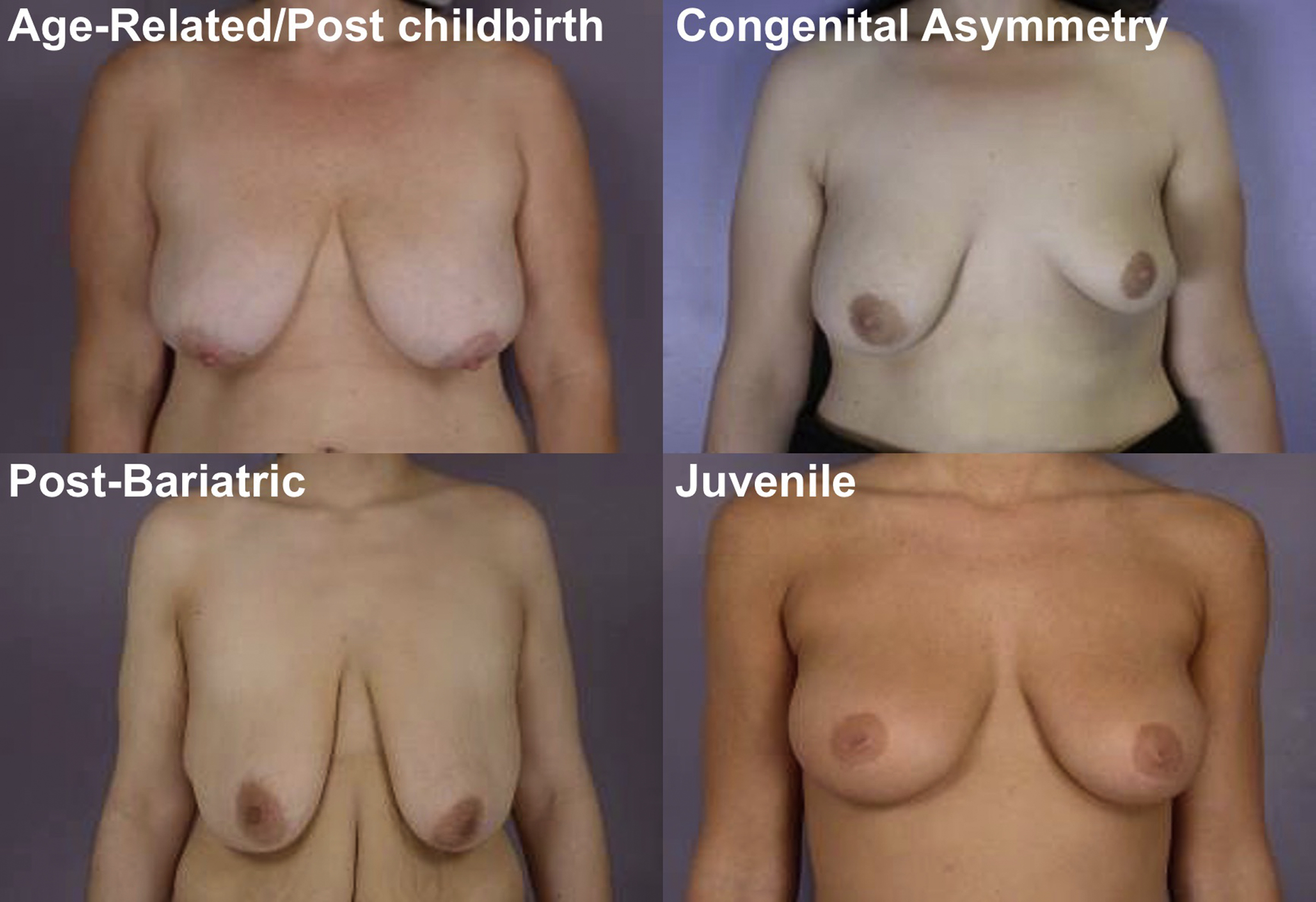
Each case presents with some differences with regards to tissue quality, concerns, and expectations. All, however, have inadequate breast volume with an excess of skin envelope, have nipple displacement, and display poor tissue quality resulting in a 3-dimensional deformity. Overlying this, there is often a significant emotional component.
To stage or not to stage: that is the question
There is a school of thought to always stage these procedures based on the proposal that the combined operation has a high complication rate and a high rate of patient dissatisfaction. The well-known “Surgeon Beware” article by Dr Spear caused many people to reconsider whether they would perform augmentation mastopexy as a combined procedure. However, articles by Calobrace and colleagues and Stevens and colleagues refuted this assertion with data based on their practices. These articles demonstrated that the reoperation rate is not significantly higher than the additive for performing the two procedures independently with the mastopexy-only reoperation rate of 10.2% comparable to the tissue-related reoperation rate of augmentation mastopexy of 13.3%. This has been the experience in the author’s practice. Despite this, there are certainly patients who are not suitable for a combined single-stage procedure. The first group are those patients with extremely poor tissue quality who often also have very poor inframammary fold fixation. Typical of this patient would be a massive weight loss with an sternal notch:nipple distance of 35 cm, lateralized nipples, poor IMF fixation, poor tissue quality, and severely volume-depleted breasts. This situation is not confined to the massive weight loss patient but is typical in that situation. There are also patients at the other end of the spectrum with significant breast tissue in whom it is borderline as to whether they need or desire an implant ( Fig. 2 ). In these cases, it is sometimes also worthwhile staging the patient and allowing a reassessment as to the need for an implant 3 months after the mastopexy. Patients with significant asymmetry are best staged to attain symmetry at an initial stage and then use symmetric augmentation at a second stage. This limits the risk of the breasts behaving differently over time because of the different ratio of implant to native tissue.

Principles of single stage augmentation mastopexy
This procedure requires the following:
- 1.
An increase in the volume in the upper pole
- 2.
A decrease in the horizontal excess in the lower pole
- 3.
A decrease in the vertical excess in the lower pole
- 4.
A repositioning of the nipple to an aesthetically pleasing position
- 5.
Protection of the T-junction
- 6.
Creation of a defined stable fold
To achieve this, one needs to
- 1.
Use a moderate implant size
- 2.
Attempt to apply the 14-point plan, that is, good augmentation technique
- 3.
Modify the breast to reshape over the new volume, not just tighten the skin
- 4.
Appropriately modify the nipple position
- 5.
Avoid a T-junction of breast tissue while reconfiguring the breast tissue in a manner that maximizes aesthetics and minimizes the risk of a waterfall deformity (breast-implant mismatch) or bottoming out (lower pole stretch deformity).
Planning
Implant Selection
Shape
In general, the author prefers to use round implants for augmentation mastopexy, as he is trying to achieve upper pole fullness, and accurate pocket control can be slightly more difficult in this circumstance. The use of anatomically shaped implants in this instance would theoretically lead to an increased risk of rotation as well as the risk of anaplastic large cell lymphoma, which must be considered (see later discussion).
Size
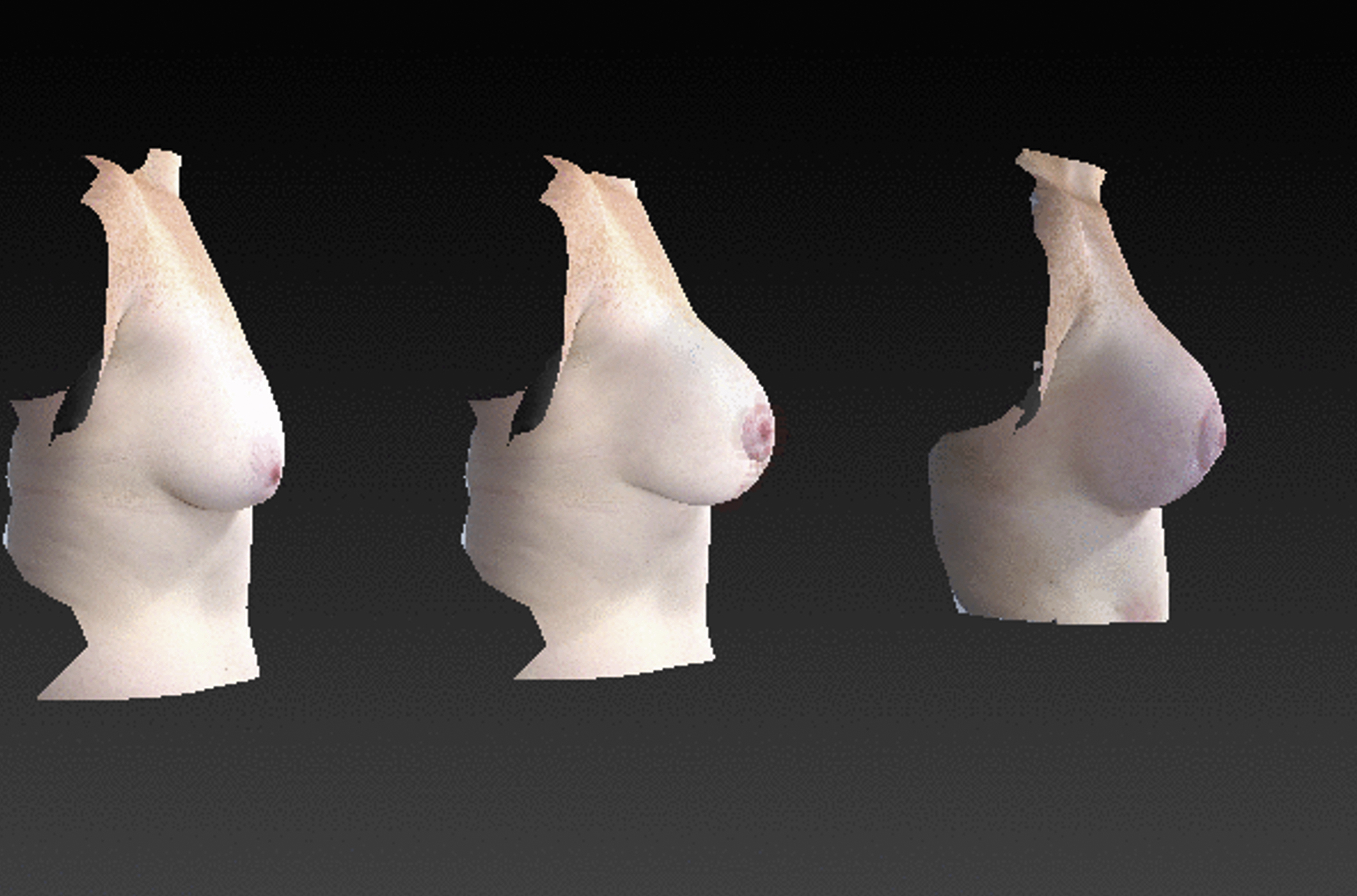
Sizing is based on the principles of dimensional planning with the base dimension and the projection giving final volume. The appropriate base dimensions for the implant are measured to obtain an aesthetically pleasing take-off point superiorly and with appropriate width. The author tends to favor moderate projecting implants, as the coning effect of the pillar approximation tends to cause an increase in breast projection, and the use of high projecting implants further increases the projection, potentially resulting in an overprojecting, abnormally shaped breast. The added volume also adds weight and increases the risk of secondary bottoming out/stretch deformity. Communicating this sizing with the patient can be relatively difficult in the augmentation mastopexy patient, as the presence of ptosis often gives the illusion of size that is not present. Most plastic surgeons have seen patients who present wanting a breast reduction who in the end need a mastopexy with augmentation because they have little tissue, but the sag gives the false impression of greater size. The use of sizers and a bra generally significantly overestimates the size, and the author has found the patient can find this somewhat off-putting. He has found the use of high-quality 3-dimensional imaging and simulation (Vectra – Canfield scientific, or similar) to be invaluable. In the absence of this, the best option is to use dimensional planning for base width and moderate projecting implants ( Fig. 3 ).
Texture
In many jurisdictions, the use of textured implants has been dominant until the recent increase of concerns regarding breast implant associated – anaplastic large cell lymphoma (BIA-ALCL) with the primary advantage of pocket stability in a patient who already has documented poor tissue quality. Apart from BIA-ALCL, there are other potential disadvantages of textured implants with the stability of the implant potentially being out of sync with the instability of the native breast tissue resulting in the potential for higher incidence of waterfall deformity. The advantage of smooth-walled implants is that they may potentially autoadjust to the relaxation of the native tissues in the postoperative period. This is obviously a 2-edged sword with the potential for significant bottoming out because of less pocket stability. This is a discussion the author has with patients, and in the patient with better-quality tissues, the author generally uses smooth-walled implants. However, he considers the use of textured implants in patients with poorer tissues, but in whom it should still be reasonable to perform a single-stage procedure. In some locations, patients will not countenance the use of a textured implant, and smooth implants are the only option.
Fill
Modern cohesive silicone gel implants are the implant of choice in the author’s practice. These patients generally have poor tissue cover over the implant, and as such, the higher risk of implant rippling and palpability that needs to be mitigated.
Tissue Planning
Nipple position
Historically, there have been many approaches to determining nipple position in mastopexy, augmentation mastopexy, and breast reduction.
- •
Penn : the most aesthetic location at which nipples should be placed is at the 2 basal angles of an imaginary equilateral triangle that has its apex at the sternal notch and has sides measuring 21 cm. THAT IS, IN ALL PATIENTS THE SN:NIPPLE DISTANCE SHOULD BE 21 CM. However, he based his idea on a small sample of women between the ages of 18 and 39 years.
- •
Midhumeral point: Maliniac suggested the nipple will be above the horizontal drawn between the point midway between the acromion and olecranon, while Pitanguy recommended use of the midhumeral point plus 2 or 3 cm for determining the new nipple level. However, patients come in all shapes and sizes: low breasted, high breasted, long chested, short chested, and so forth. Augmentation mastopexy patients present at different ages and sizes and with different degrees of ptosis, IMF positions, and tissue quality. Is there any relationship between the length of the arm and the position of the breast on the chest and the position of the nipple on the breast?
- •
IMF projected onto the anterior breast is very operator dependent and can be difficult to teach. It was initially used for inferior pedicle breast reduction, where there tends to be more bottoming out and lower pole stretch; hence, it may leave the nipple low for other techniques, such as superomedial pedicle or in augmentation mastopexy.
- •
Hands-on-head technique: In breast augmentation, the predicted nipple position is fixed, and the implant vertical position and lower pole skin cover are adjusted to achieve an appropriate nipple position on the new breast. The future nipple position can be predicted by lifting the arms at 45° or simply “hands on the head.” With Per Heden’s maneuver (which is widely published in his numerous articles), he theoretically simulates the nipple shift after the implant placement. In mastopexy, augmentation/mastopexy and breast reduction the position of the nipple can be chosen based on position or expected position of the IMF and adjusting the nipple position in a reverse manner to that used for augmentation. The author generally uses this position as the top of the areola rather than the actual nipple position to account for a degree of expansion of the lower pole in the postoperative period (better a little low than too high!) ( Figs. 4–6 ).

Fig. 4
The current IMF is transferred to the midline.
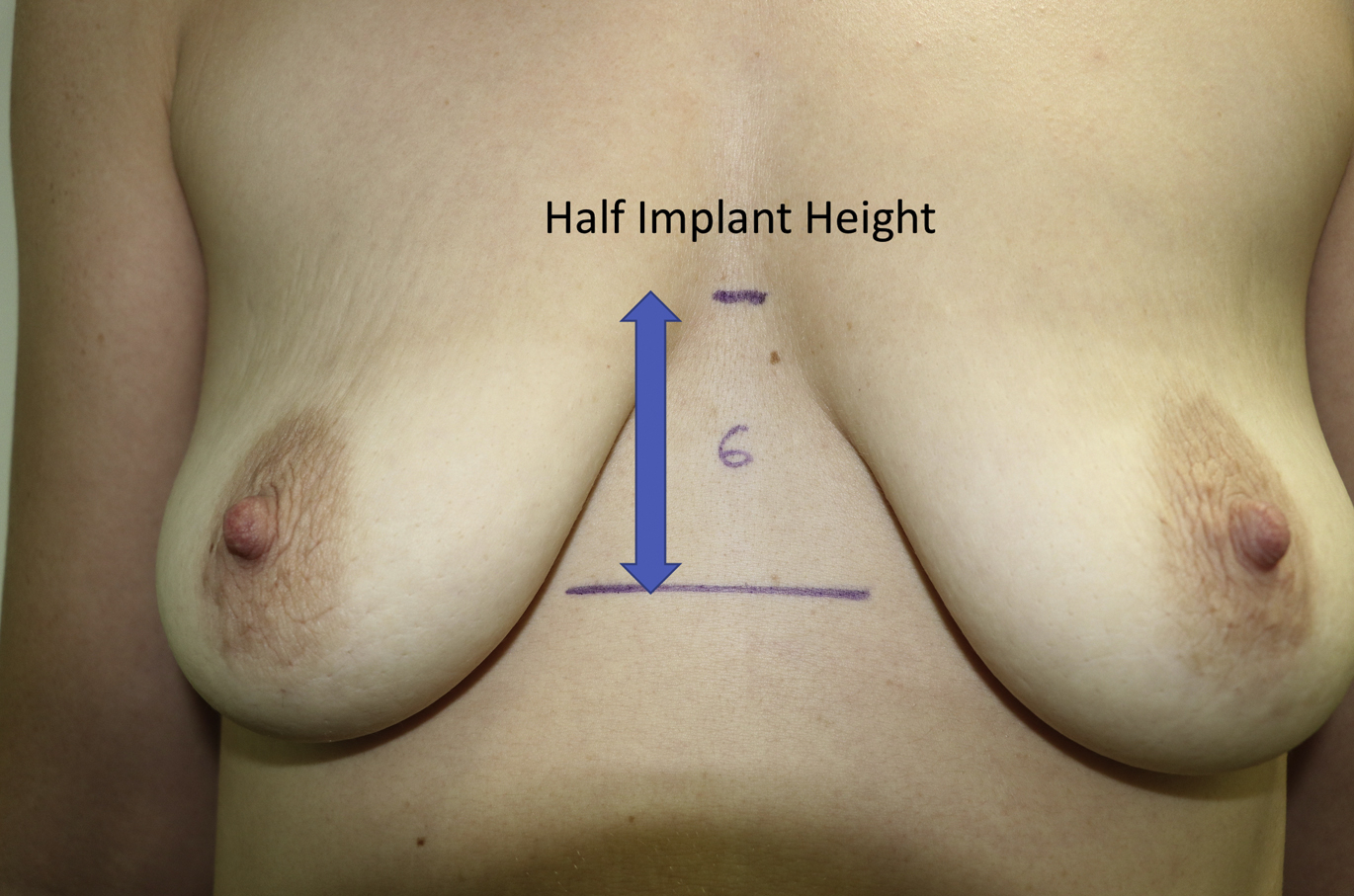
Fig. 5
A mark is made half the implant height above the IMF mark.
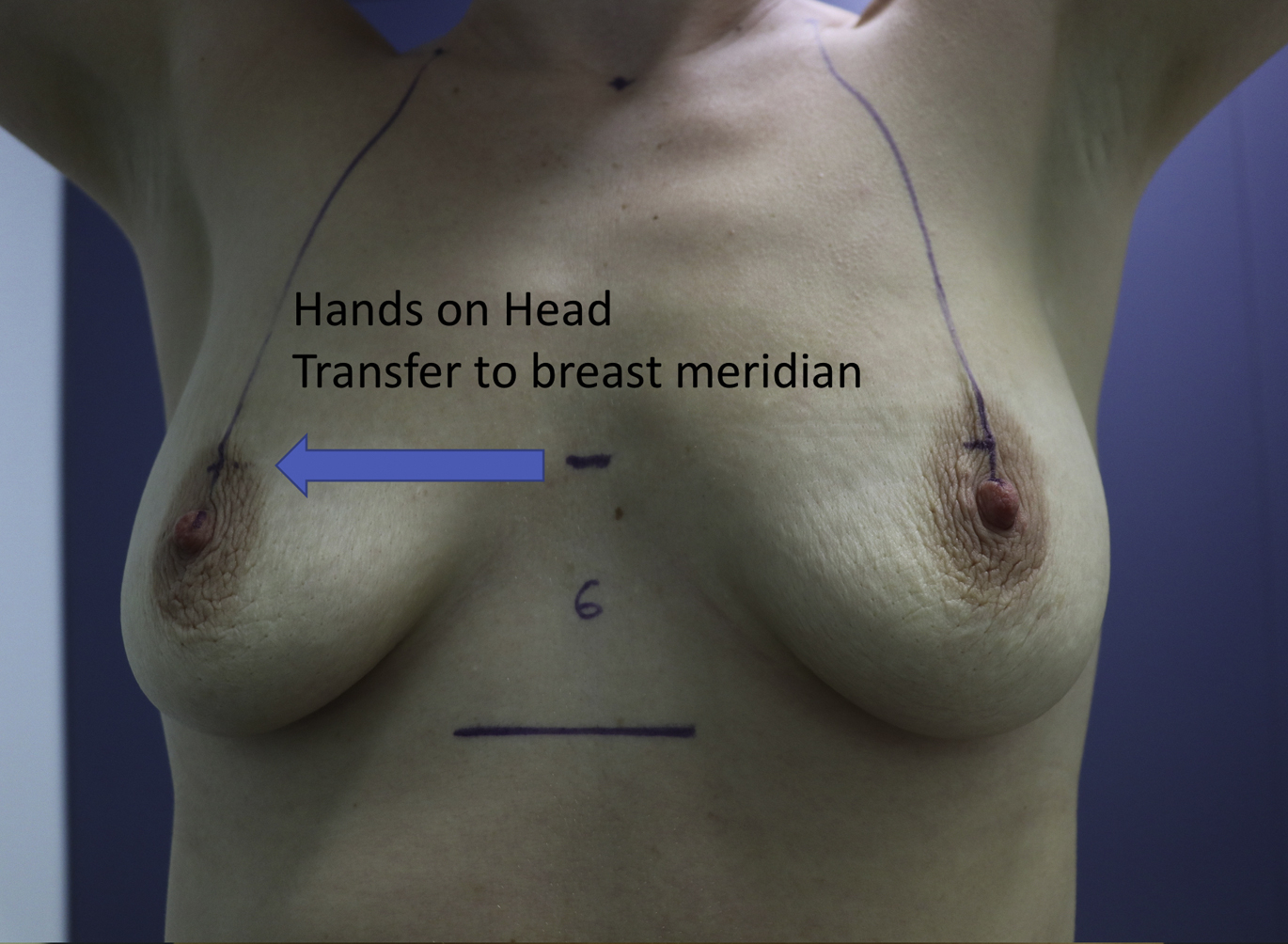
Fig. 6
With the hands on the head, the new nipple position is transferred to the breast meridian.
Other Markings
Once the nipple position is determined, the vertical limbs of the mastopexy are planned in the usual fashion by rotating the lower pole of the breast to the median of the breast and drawing a vertical line. The planned implant lower and upper pole positions are marked on the sternum and extended across onto the breast using a spirit level to allow intraoperative assessment and adjustment. The vertical limb length is marked appropriately for the given implant and breast volume. There are many techniques for this. The author uses the lower ventral curvature of the implant + half the lower pole pinch thickness. Further discussion of this is beyond the remit of this article. All marks apart from the position of the IMF incision are approximations that are confirmed sequentially intraoperatively ( Fig. 7 ).
Related posts:
 Breast Implant–Associated Anaplastic Large Cell Lymphoma
Breast Implant–Associated Anaplastic Large Cell Lymphoma
 Hot Topics in Breast Surgery
Hot Topics in Breast Surgery
 Fundamentals of High-Resolution Ultrasound in Breast Implant Screening for Plastic Surgeons
Fundamentals of High-Resolution Ultrasound in Breast Implant Screening for Plastic Surgeons
 Moving Toward Opioid-Free Breast Surgery
Moving Toward Opioid-Free Breast Surgery
 An Algorithm for the Management of Explantation Surgery
An Algorithm for the Management of Explantation Surgery
 The Use of Anatomic Implants in Aesthetic Breast Surgery
The Use of Anatomic Implants in Aesthetic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


