div class=”ChapterContextInformation”>
9. Alopecia Areata: Clinical Treatment
Keywords
Alopecia areataTreatmentSteroidsClobetasolIntralesional steroidsSystemic steroidsPrednisonePrednisoloneDexamethasonePulse therapyTopical immunotherapySquaric acid2,3-Dyphenylcyclopropenone (DPCP)AnthralinPhototherapyExcimer laserUVA-1UVB-nbCyclosporineMethotrexateAzathioprineSulfasalazineJAK inhibitorsTofacitinibRuxolitinibBaricitinibMinoxidilProstaglandin F2a analogsVitamin D3Ezetimibe/simvastatinPlatelet-rich plasmaFexofenadineEbastineAromatherapyLatanoprostBimatoprostTravoprostHow to Choose the Best Treatment for Your Patient?
- 1.
Age of the patient: Some systemic medications may represent an unjustified risk in the pediatric population. In addition, children have low tolerance to pain and treatment such as intralesional steroids can cause a lot of stress. On the other hand, geriatric patients may use a number of drugs, and clinicians should be aware of possible interactions.
- 2.
Extent of the disease: While localized disease may improve spontaneously or with local treatments, extensive alopecia usually requires the use of systemic drugs or immunotherapy.
- 3.
Disease progression: Active and rapidly progressive disease may benefit from more aggressive interventions such as oral steroids or immunosuppressants.
- 4.
Personal coping with disease: Emotional support increases compliance to treatment. Understanding the patients’ needs will help in choosing the best treatment plan. Dedicating some time to discussing camouflage options, patient support organizations, and psychological/group therapy may provide great help for the patient (Fig. 9.1).
- 5.
Compliance: Treatment success requires good compliance. Some treatments can be done at home but may require daily application of topicals; other treatments can be done at the office but require frequent visits. Patients and doctor should discuss realistic options.
- 6.
Cost of medication/insurance coverage: Treatment of alopecia areata is often long lasting, and the disease frequently relapses. This topic is clearly of utmost importance for treatment adherence.

A patient with alopecia areata totalis treated with scalp micropigmentation
Treatment in alopecia areata in children and adults
Age 0–10 years old | Age > 10 years old |
|---|---|
Localized a First line: Topical corticosteroids or excimer laser Second line: Topical immunotherapy, anthralin, or phototherapy Extensive b First line: Topical immunotherapy, anthralin, or phototherapy Second line: Pulse systemic steroids or topical minoxidil Alopecia areata totalis/universalis First line: Topical immunotherapy or anthralin Second line: Phototherapy | Localized First line: Topical corticosteroids or intralesional corticosteroids Second line: Topical immunotherapy or anthralin Third line: Phototherapy or excimer laser Extensive First line: Topical immunotherapy, anthralin, or phototherapy Second line: Topical corticosteroids with occlusionc or pulse oral steroids Third line: Oral tofacitinib 5 mg twice a day Alopecia areata totalis/universalis First line: Topical corticosteroids with occlusionc or topical immunotherapy Second line: Oral tofacitinib 5 mg twice a day Third line: Phototherapy, combination therapyd |
Treatment alopecia areata affecting beard/eyelashes/eyebrows
Beard | Eyebrowsa | Eyelashes |
|---|---|---|
First line: Topical corticosteroids, topical minoxidil, topical prostaglandin agonistsb Second line: Phototherapy, excimer laser Third line: Topical immunotherapy, anthralin, 2% topical tofacitinib | First line: IL corticosteroidsc, topical corticosteroids, topical minoxidil, topical prostaglandin agonists. Second line: Topical immunotherapy, excimer laser Third line: 2% topical tofacitinib | First line: Topical corticosteroids, topical prostaglandin agonist Second line: 2% topical tofacitinib |
Since the cause of alopecia areata is unknown,the authors believe that there is no need for extensive laboratory or imaging studies. Association with dental “foci” or other infections has never been confirmed and screening for autoimmune diseases is not routinely necessary. Parents often ask about the risk of relapses after vaccination; the only vaccine that has been associated with onset of alopecia areata is the hepatitis B vaccine.
Steroids: Topical, Intralesional, Systemic

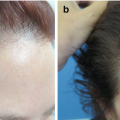
Hair regrowth with topical potent steroids under occlusion therapy. Note presence of ecchymosis due to scalp atrophy
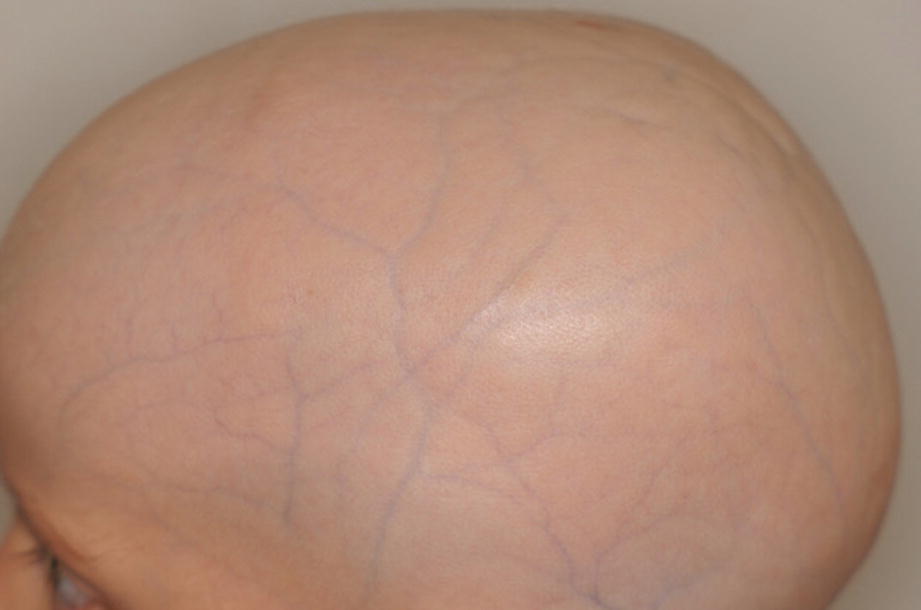
Severe scalp atrophy in a child treated with long-term topical steroids
One FTU is the amount of topical steroid that is squeezed out from a standard tube along an adult’s fingertip from the very end of the finger to the first crease in the finger and is equivalent to 0.5 g of steroid.
Intralesional steroid dosing in alopecia areata
Steroid | Dose | Efficacy | |
|---|---|---|---|
Scalp | TA | 2.5–10 mg/cca | 42.99–92% |
BD | 1.25 mg/cc | 44.4% | |
HA | 25 mg/cc | ||
Eyebrows, beard, and other body parts | TA | 2.5 mg/cc |

Scalp atrophy after intralesional steroids

Gluteal atrophy after superficial steroid injections
Systemic therapy is a possible option in case of acute rapid progressing alopecia areata. It may also be used in localized but very active cases. Systemic steroids are not a good option in alopecia totalis/universalis as response is poor. Response varies from 11% to 88%, with relapse rates of 28–100%. Side effects associated with pituitary-adrenal axis suppression prohibit long-term treatments; therefore, relapse rates are high. If you choose to use systemic steroids as an initial approach, you need to plan maintenance with other systemic/local treatments with a better safety profile. Pulse therapy is the preferred treatment, but there are no studies comparing results with different steroids or regimens. Always prescribe alendronate, calcium, and vitamin D3 when you prescribe systemic steroids for more than 1 month to prevent osteoporosis.
Oral steroid therapy
Scheme | Efficacy | Relapse | |
|---|---|---|---|
Prednisone | 5 mg/kg (300 mg) oral prednisone once a month for 3–6 months | 82% | 0% |
Dexamethasone | Dexamethasone 2 mg twice a week for 6 months | 75% | 16% |
Dexamethasone 0.5 mg/day for 6 months | 37% | 75% | |
Prednisolone | 80 mg for 3 consecutive days once every3 months | 66% | 33% |
300 mg pulses at 4-week intervals | 58% | N/A | |
200 mg once weekly | 34% | 25% | |
0.5 g daily for 5 days | 11% | N/A | |
1000 mg pulses (AA totalis and universalis) | 42% | N/A |
Intramuscular steroid therapy
Scheme | Efficacy | Relapse | |
|---|---|---|---|
Triamcinolone | 40 mg once a month for 6 months followed by 40 mg once every 1.5 months for 1 year | 74% | 46% |
40 mg every 4 weeks for a maximum of 6 months, followed by immunotherapy to reduce relapse | 63% | 47.11 |
Intravenous steroid therapy
Efficacy rate | Relapse rate | ||
|---|---|---|---|
Methylprednisolone | Adults: 500 mg QD or 250 mg BID over a period of 1 hour on 3 consecutive days per month for three courses | 20–80% | 16.7–100% |
Children: 8–20 mg/kg over a period of 1 hour on 3 consecutive days per month for three courses | 25–67% | 40–81% | |
Prednisolone | Adults: 100 mg QD on 3 consecutive days per month for three courses | 73% | 30% |
Adults: 2 g single-dose IV | 11% | N/A |
Corticosteroid-Sparing Agents/Disease-Modifying Antirheumatic Drug (DMARD)
Since systemic corticosteroids are not recommended for long-term treatment, different corticosteroid-sparing agents may be used. The main action of these agents involves the inhibition of lymphoid proliferation. Cyclosporine (Cya), methotrexate, and azathioprine have shown different levels of efficacy as both monotherapy and combination therapy with systemic steroids. The authors rarely utilize Cya because dosages required to treat alopecia areata are high (6 mg/kg/day), results are not consistent, and the safety profile is a concern. We utilize methotrexate (15 mg a week plus folic acid) in association with systemic steroids, keeping in mind that results from this treatment are not fast. We don’t have personal experience with sulfasalazine, which has been utilized with success in some studies [5–11]. Mycophenolate mofetil and topical calcineurin inhibitors are not effective.
Monotherapy with corticosteroid-sparing agents
Dose | Duration | Efficacy | Relapse | Side effects | |
|---|---|---|---|---|---|
Cyclosporine | 6 mg/kg/day | 3–27 months | 50–53% | 20–100% | Gastrointestinal symptoms, hypertrichosis, hypertension, weight gain, headache/dizziness, nephrotoxicity |
Methotrexate | 10–15 mg/week | 28 weeks | 64–89% | 31–73% | Transient elevated transaminases, persistent nausea, and lymphocytopenia |
Azathioprine | 2.5 mg/kg/day | 10 months | 43% | 14.30% | Diarrhea, elevation of liver enzymes, pancreatitis, and bone marrow suppression |
Sulfasalazine | 3 g/day | 6 months | 25.60% | N/A | N/A |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


