Antia-Buch Flaps for Ear Reconstruction
Amir M. Ghaznavi
Brian R. Gastman
DEFINITION
Antia-Buch flaps are best used for traumatic or postsurgical helical defects of the upper third and middle third of the ear that measure between 25% and 50% of length of the helix.1
ANATOMY
The ear is made up of delicate skin and soft tissues covering a cartilaginous framework and underlying muscles.
The cartilaginous portion of the ear includes the conchal bowl, antihelix, and helix.
The surrounding muscles of the ear can be divided into intrinsic muscles (muscles that originate and insert on the ear) and extrinsic muscles (muscles that originate in other regions of the skull and insert onto the ear).
The intrinsic muscles include the helicis major, helicis minor, tragicus, antitragicus, transverse, and oblique muscles.
The extrinsic muscles include the anterior, superior, and posterior auricular muscles.
The arterial supply of the ear is derived from the posterior auricular artery and perforators arising from the superficial temporal artery.
Venous drainage is provided by the posterior auricular veins that drain into the external jugular system as well as the superficial temporal and retromandibular veins.
Lymphatic drainage of the ear is to the parotid, infraclavicular, mastoid, and infraauricular cervical nodes.
Sensory innervation of the ear is provided by:
1. Great auricular nerve (C2-C3)
Auriculotemporal nerve (V3)
Lesser occipital nerve
Auricular branch of the vagus nerve (Arnold nerve)
PATIENT HISTORY AND PHYSICAL FINDINGS
A complete history and physical exam of the head and neck should be performed to document the exact location of the defect within the ear (superior third, middle third, and lower third portions) and involvement of cartilage if present.
The patient should also be examined for evidence of nodal metastases and secondary lesions in the head and neck region. Attention should be paid to the lymph node basins in the parotid and cervical areas.
Comorbidities that can increase the risk of postoperative wound healing and bleeding complications should be evaluated and optimized if possible.
IMAGING
No imaging is required for Antia-Buch flaps; however, imaging of the head and neck region may be necessary to evaluate tumor metastasis.
NONOPERATIVE MANAGEMENT
Isolated skin defects of the helical rim with intact underlying cartilage and perichondrium can heal by secondary intention or full-thickness skin grafting.
Full-thickness skin grafts can result in excellent outcomes in patients with preserved cartilaginous support. However, healing by secondary intention or skin grafting of more complex lesions that include full-thickness excision of the underlying cartilage may result in contour abnormalities and require more complex reconstructions.
SURGICAL MANAGEMENT
Preoperative Planning
The contours of the ear are marked preferably before skin prep to avoid washing off.
Patients who have large defects of the ear should be counseled that they may require contralateral reduction by wedge resection and/or setback of the unaffected ear at a later time to obtain symmetry.
Positioning
The patient is placed in a supine position with the entire ear exposed including the hairline.
The bed is turned 180 degrees to allow unimpeded approach to the head and neck area.
The contralateral ear may be exposed if planning on contralateral procedure and to evaluate symmetry.
Approach
Several surgical approaches have been described for Antia-Buch flaps including those for “classic” helix-only defects that are less than 25% of the total length of the helix, as well as modifications for longer defects and defects that include loss of the helix, scapha, and antihelix.
Prophylactic antibiotics are administered by most surgeons particularly if the cartilage or perichondrium has been removed.
Coverage with fluoroquinolones provides excellent cartilage penetration and provides coverage of common organisms that can cause infections of the ear (eg, Pseudomonas aeruginosa).
Prolonged antibiotic treatment is usually not necessary unless the wound is contaminated or the patient is otherwise at risk for postoperative infections.
TECHNIQUES
▪ “Classic” Helix-Only Defect1
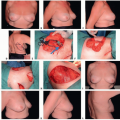
The lesion and the proposed area of resection are identified and marked on the ear (TECH FIG 1A).
The resection is performed with an incision in the helical sulcus to remove the lesion and separate the helical cartilage from the scapha (TECH FIG 1B).
An incision is made in the helical sulcus (either inferiorly, superiorly, or both) extending through the anterior skin and cartilage taking care to avoid injury to the postauricular skin.
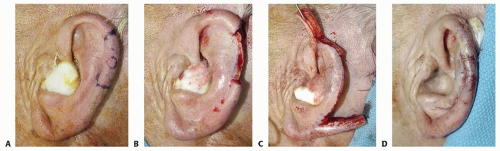
TECH FIG 1 • A. Helix defect marked. B. Helix freed from scapha. C. Formation of chondrocutaneous composite flaps superior and inferior. D. Composite flaps advanced and closed.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access