Flap |
|
Tissue |
Fasciocutaneous as perforator/myocutaneous |
Course of the vessels |
Base of the intermuscular space between the rectus femoris muscle and the vastus lateralis muscle |
Dimensions |
Maximum 20 × 10 cm; greatly dependent on the inclusion of the ABC perforators |
Extensions and combinations |
ALT/TFL, ALT/vastus lateralis, ALT/iliac crest, ALT/AMT |
Anatomy |
|
Neurovascular pedicle |
— |
Artery |
Descending branch of the lateral circumflex femoral artery |
Veins |
Two concomitant veins |
Length and arc of rotation |
8–16 cm depending on point |
Diameter |
2–2.5 cm below rectus femoris branch; 2.5–3.5 cm above rectus femoris branch |
Nerve |
Lateral femoral cutaneous/lateral branch |
Surgical technique |
|
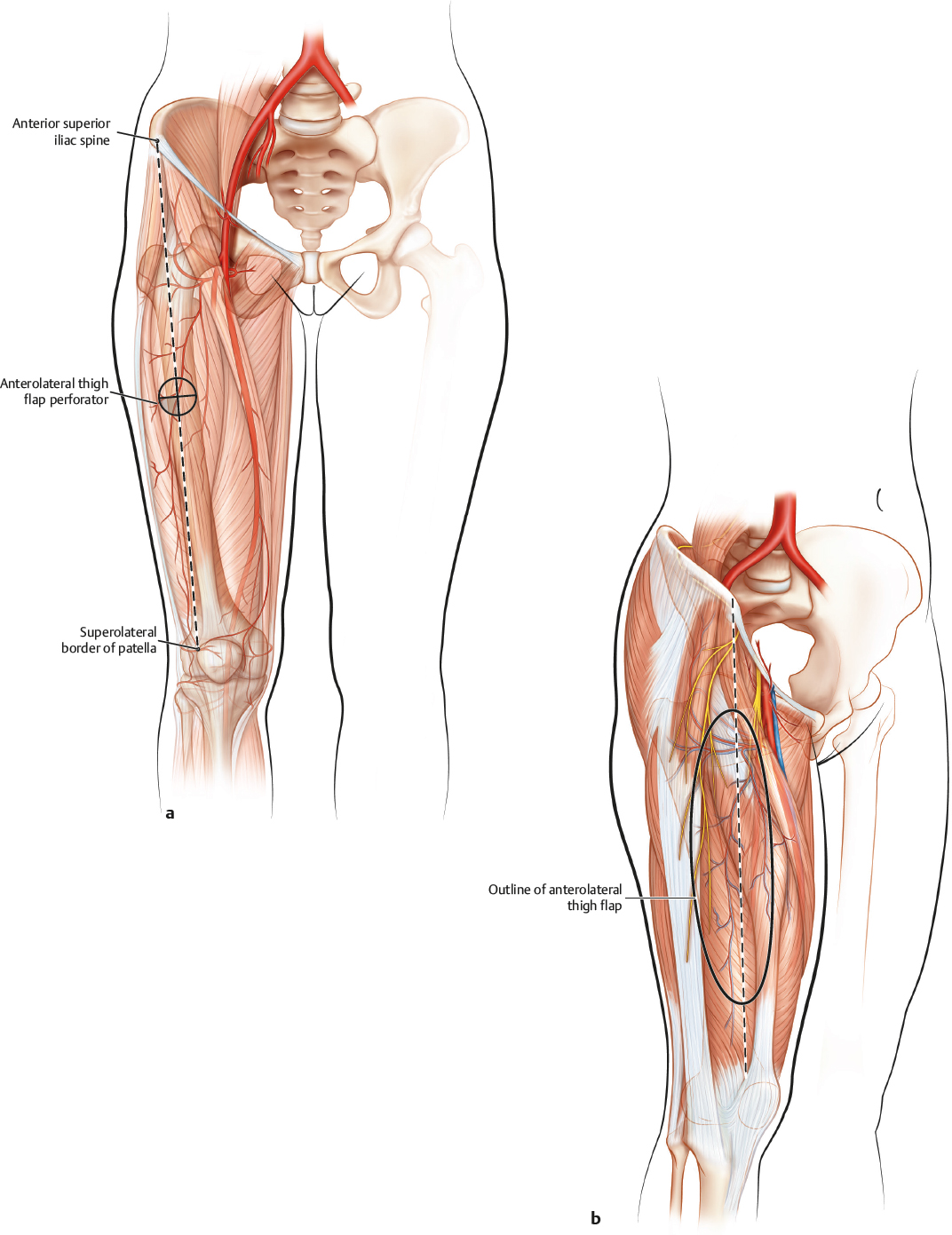
Preoperative examination and markings |
Straight line drawn from the anterior superior iliac spine to the upper/outer margin of the patella; Doppler confirmation of perforator B just lateral to halfway point; Doppler confirmation of perforators A and C 5 cm above and below perforator B, respectively |
Patient position |
Supine neutral position feet straight up |
Dissection |
Begin with a curvilinear incision 1.5–2 cm medial to the anterior superior iliac spine/patellar line from a point proximal to perforator A to a point distal to perforator C; depth of dissection should be subfascial, moving from medial to lateral; retracting the rectus femoris medially will expose the descending branch of the lateral circumflex femoral pedicle; identify the appropriate perforators exiting the pedicle and determine their route to the surface; if confined to the septum, visualize their travel and ensure their continuity to the overlying skin paddle; in a majority of cases, the perforators will travel through the vastus lateralis and must be carefully dissected out of and away from the muscle; in this case, dissection is usually directed from superficial to deep; all intramuscular branches should be mechanically or thermally ligated
When the perforators travel deeper within the muscle, it may be prudent to include a cuff of the muscle around the perforator; after concluding the dissection to the cutaneous island, the lateral curvilinear incision may be completed to the design needs of the recipient defect; the distal extent of the pedicle should be divided and the main vessels dissected proximally until sufficient length is attained; preservation of the co-located motor nerve is strongly recommended |
Advantages |
|
Vascular pedicle |
Generous length, large caliber, reliable location |
Flap size and shape |
Large, elliptical skin paddle |
Combinations |
May be raised with the TFL and/or the vastus lateralis muscle |
Donor site |
Minimal to no functional deficit; aesthetically favorable as compared with most other cutaneous flap donor sites |
Disadvantages |
|
Donor site morbidity |
Large flap donor sites may require skin graft closure |
Dissection |
Perforator continuity must be confirmed before cutaneous flap dissection can be completed; perforator and travel are highly variable |
Flap |
Thickness may present a problem in overweight patients |
Pearls and pitfalls |
|
Dissection |
Do not make the initial skin incision too laterally; be patient when determining the course and travel of the chosen perforator; do not isolate the cutaneous flap until the route of the perforators is ensured |
Extensions and combinations |
Including the TFL requires the inclusion of the transverse branch of the lateral circumflex femoral vessels |
Contouring and correction |
Thinning the flap is possible |
Clinical applications |
Wide variety of uses, including the head and neck, trunk, and upper and lower extremities |