14
Anterior Interosseous Nerve Syndrome
Michael F. Bothwell and Kevin D. Plancher
History and Clinical Presentation
A 28-year-old weight lifter presents with weakness in his ability to pinch over the last 6 months after having an interscalene block for shoulder surgery. He also reports an ache in his forearm but no other pain or numbness. The patient is an avid weight lifter but reports no specific trauma or previous history of problems in the same area.
Physical Examination
When a patient is asked to pinch, active flexion of the distal interphalangeal (DIP) index is impossible (Fig. 14–1). There is an inability to flex the interphalangeal joint of the thumb and the distal phalangeal joint of the index finger secondary to weakness of the flexor pollicis longus (FPL) and the index flexor digitorum profundus (FDP), with weakness of the pronator quadratus. A positive Tinel’s test over the proximal forearm is also seen with pain radiating distally. The patient reports intermittent pain in the proximal portion of the volar forearm, with no atrophy or sensory changes.
PEARLS
- Accurate attempt at pinch by patient is crucial to diagnosis—“OK” sign tip to tip.
- Weight lifters often have hypertrophy of the forearm muscles leading to this diagnosis.
- Complete hemostasis is essential during surgery with tourniquet, but limit time to ensure speedy recovery.
PITFALLS
- Inaccurate diagnosis can lead to unnecessary surgery.
- Understanding anatomy in the forearm is crucial to successful recovery.
- Position of the patient’s neck in shoulder surgery should be monitored by the anesthesiologist and surgeon.
Differential Diagnosis
- Isolated rupture of the flexor pollicis longus (FPL)
- Rupture of the index flexor digitorum profundus (FDP)
- Laceration of the nerve
- Tumor of the forearm
- Anterior interosseus nerve palsy
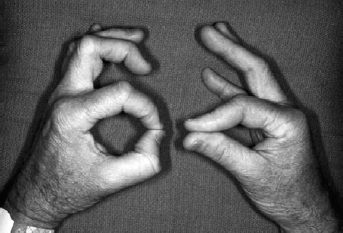
Figure 14–1. Typical pinch sign with flattening of index pulp and classic palsy of the anterior interosseous nerve with “ok” sign on left hand.
Diagnostic Studies
Electromyogram (EMG) will confirm the diagnosis of anterior interosseous nerve syndrome (AINS) in most cases if the test is focusing on the individual muscles, FPL/FDP index, and pronator quadratus. Nerve conduction tests are often normal. X-rays should also be taken to ensure there is no underlying cause or fracture.
Diagnosis
Anterior Interosseous Nerve Palsy
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


