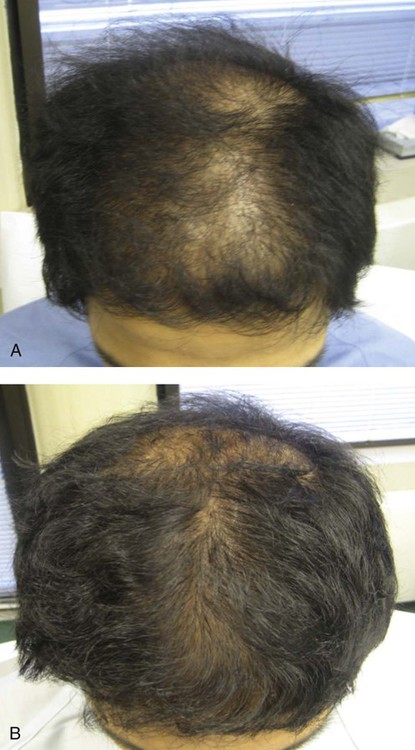
12 Androgenetic alopecia Walter P. Unger, Robin H. Unger and Carlos K. Wesley Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Since the 1940s, male pattern baldness (MPB) has been recognized as an androgen-dependent condition. Eventually, dihydrotestosterone (DHT) was established as the key androgen involved in (a) the shortening of the anagen growth phase, and (b) the progressive follicular miniaturization that accompanies each hair growth, loss, and regrowth cycle – the two hallmarks of MPB. The role of androgens in female pattern hair loss (FPHL), however, remains uncertain and prevents us from defining pattern hair loss in both genders as androgenetic alopecia (AGA). Both MPB and FPHL are often familial and have a polygenetic inheritance pattern. Management strategy Accurate diagnosis is a prerequisite for the effective treatment of MPB and FPHL. Alternative causes of alopecia that may mimic pattern hair loss must be ruled out and include diffuse alopecia areata, hair loss secondary to metabolic derangements, telogen effluvium, as well as other forms of temporary alopecia. Once this is accomplished through a review of patient history, clinical findings, and laboratory analyses, the objectives of stopping hair loss and promoting regrowth may be addressed. Men may begin experiencing MPB any time after puberty. The frequency and severity increase with age, resulting in nearly 80% of Caucasian men having some degree of MPB by age 70 years. MPB may involve bitemporal, frontal, mid-scalp, or vertex scalp areas, and is most often described according to Hamilton–Norwood patterns of severity, though Bernard Cohen’s more recent classification is more scientifically useful. FPHL tends to occur in either a ‘Ludwig type’ of diffuse central thinning or in a ‘Christmas tree’ pattern, with the wide base of the ‘tree’ located just posterior to the frontal hairline. Dawber found that 87% of a clinic sampling of premenopausal women without hair loss as a complaint had Ludwig type I–III loss. A male pattern of hair loss may also occur in women, with 79% of postpubertal women developing Hamilton type II MPB that progresses to Hamilton–Norwood type IV MPB in 25% by age 50 years, and in 50% of them by age 60 years. Medical therapy is appropriate first-line management for both MPB and FPHL. The goal is to slow the rate of hair loss and/or to reverse the miniaturization process. Currently, two medications have been approved by the US Food and Drug Administration (FDA) for these purposes: topical minoxidil (a biological response modifier) and oral finasteride (a hormone modifier). Topical 2–5% minoxidil increases the duration of the anagen hair growth phase, enlarges miniaturized follicles, and has a vasodilatory effect. Application of 1 mL to the scalp twice daily results in peak hair growth after 26–52 weeks, with the ‘crown’ showing the best response and the frontal area the least. Although 5% minoxidil is superior to 2% in increasing hair count and hair weight for MPB, adverse dermatologic effects, most commonly scalp irritation, are more common with the 5% solution (a side effect seen less frequently when the 5% is in a ‘foam’ base used once daily as compared to 2% topical solution used twice daily). Currently, only the 2% strength is FDA approved for use on women. Cessation of treatment results in reversal of the positive effect within 4 to 6 months. Anecdotally, combining topical minoxidil with finasteride sometimes produces superior results to those seen with either of these medications alone. Finasteride is a competitive inhibitor of type II 5α-reductase, the enzyme involved in converting testosterone to its metabolite, DHT. An almost 70% reduction in serum and scalp DHT levels can be achieved with 1 mg/day finasteride therapy in men. In clinical trials of crown MPB, after 5 years hair counts were increased in 65% of the subjects (versus 0% of those on placebo), and further loss was slowed or stopped in 90% (versus 25% of the corresponding placebo group). In other studies, the best response was again seen in the crown and the least in the frontal area. Dutasteride, a dual inhibitor of both type I and type II 5α-reductase, has also been demonstrated to be well tolerated and effective in improving hair growth for patients with MPB. Although data are sparse, menopausal status, circulating androgen concentrations, and hyperandrogen symptoms do not appear to predict females’ response to finasteride – a known teratogen that is contraindicated in pregnancy. Side effects in men are infrequent, affecting less than 2% of patients. Despite the fact that they are generally reversed after discontinuation of the drug and often resolve during continued treatment, on April 11, 2012, the FDA amended professional labels for finasteride to reflect the reported continuation of erectile dysfunction, ejaculation disorders, and decreased libido after discontinuation of the drug. A 7-year clinical trial demonstrated a 24.8% reduction in the overall incidence of prostate cancer in patients on finasteride versus the placebo. Subsequent analyses revealed finasteride-related risk reductions of 30% for prostate cancer in general and 27% for high-grade prostate cancer, as well as suggesting increased prostate biopsy sensitivity with finasteride use. Although there is a dearth of well-controlled clinical trials involving other anti-androgens, such as spironolactone and cyproterone acetate, in women, it appears that the value of these medications is most pronounced in those with hyperandrogenism. Fortunately, for many patients with MBP and FPHL who are refractory to medical therapy, advances in surgical techniques make hair transplantation a reliably effective option (as seen in the accompanying figure of a 26-year-old with MPB (A) before and (B) 1 year after a 2649-follicular unit transplantation). The perfecting and worldwide adoption of ‘follicular unit transplantation’ (FUT) has yielded natural-appearing results combined with cosmetically good hair density per session, that was not possible until approximately 7 to 10 years ago. Improvements in the surgical approach now allow many female patients, as well as men in the early stages of MPB, to benefit from this procedure. Furthermore, ‘pluggy’ transplants that resulted from older forms of transplantation can now often be ‘retrofitted’ to make them appear natural, and areas of cicatricial alopecia secondary to disease, trauma, or cosmetic surgery can also be considerably improved. In addition, cosmetic aids can improve the appearance of patients with hair loss if medical treatments are either ineffective, not indicated, or if they are simply preferred as an adjuvant by the patient. Thinning hair can be camouflaged by coloring the scalp with tinted powders or sprays, as well as by the wearing of wigs and hair pieces. On the other hand, hair ‘extension,’ in which bunches of hairs are attached to individual scalp hairs, is generally discouraged owing to the potential for the development of permanent scarring traction alopecia. Only gold members can continue reading. Log In or Register to continue Related Related posts: Discoid lupus erythematosus Mucoceles Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Stay updated, free articles. Join our Telegram channel Join Tags: Treatment of Skin Disease Comprehensive Therapeutic Strategies Aug 7, 2016 | Posted by admin in Dermatology | Comments Off on Androgenetic alopecia Full access? Get Clinical Tree
12 Androgenetic alopecia Walter P. Unger, Robin H. Unger and Carlos K. Wesley Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Since the 1940s, male pattern baldness (MPB) has been recognized as an androgen-dependent condition. Eventually, dihydrotestosterone (DHT) was established as the key androgen involved in (a) the shortening of the anagen growth phase, and (b) the progressive follicular miniaturization that accompanies each hair growth, loss, and regrowth cycle – the two hallmarks of MPB. The role of androgens in female pattern hair loss (FPHL), however, remains uncertain and prevents us from defining pattern hair loss in both genders as androgenetic alopecia (AGA). Both MPB and FPHL are often familial and have a polygenetic inheritance pattern. Management strategy Accurate diagnosis is a prerequisite for the effective treatment of MPB and FPHL. Alternative causes of alopecia that may mimic pattern hair loss must be ruled out and include diffuse alopecia areata, hair loss secondary to metabolic derangements, telogen effluvium, as well as other forms of temporary alopecia. Once this is accomplished through a review of patient history, clinical findings, and laboratory analyses, the objectives of stopping hair loss and promoting regrowth may be addressed. Men may begin experiencing MPB any time after puberty. The frequency and severity increase with age, resulting in nearly 80% of Caucasian men having some degree of MPB by age 70 years. MPB may involve bitemporal, frontal, mid-scalp, or vertex scalp areas, and is most often described according to Hamilton–Norwood patterns of severity, though Bernard Cohen’s more recent classification is more scientifically useful. FPHL tends to occur in either a ‘Ludwig type’ of diffuse central thinning or in a ‘Christmas tree’ pattern, with the wide base of the ‘tree’ located just posterior to the frontal hairline. Dawber found that 87% of a clinic sampling of premenopausal women without hair loss as a complaint had Ludwig type I–III loss. A male pattern of hair loss may also occur in women, with 79% of postpubertal women developing Hamilton type II MPB that progresses to Hamilton–Norwood type IV MPB in 25% by age 50 years, and in 50% of them by age 60 years. Medical therapy is appropriate first-line management for both MPB and FPHL. The goal is to slow the rate of hair loss and/or to reverse the miniaturization process. Currently, two medications have been approved by the US Food and Drug Administration (FDA) for these purposes: topical minoxidil (a biological response modifier) and oral finasteride (a hormone modifier). Topical 2–5% minoxidil increases the duration of the anagen hair growth phase, enlarges miniaturized follicles, and has a vasodilatory effect. Application of 1 mL to the scalp twice daily results in peak hair growth after 26–52 weeks, with the ‘crown’ showing the best response and the frontal area the least. Although 5% minoxidil is superior to 2% in increasing hair count and hair weight for MPB, adverse dermatologic effects, most commonly scalp irritation, are more common with the 5% solution (a side effect seen less frequently when the 5% is in a ‘foam’ base used once daily as compared to 2% topical solution used twice daily). Currently, only the 2% strength is FDA approved for use on women. Cessation of treatment results in reversal of the positive effect within 4 to 6 months. Anecdotally, combining topical minoxidil with finasteride sometimes produces superior results to those seen with either of these medications alone. Finasteride is a competitive inhibitor of type II 5α-reductase, the enzyme involved in converting testosterone to its metabolite, DHT. An almost 70% reduction in serum and scalp DHT levels can be achieved with 1 mg/day finasteride therapy in men. In clinical trials of crown MPB, after 5 years hair counts were increased in 65% of the subjects (versus 0% of those on placebo), and further loss was slowed or stopped in 90% (versus 25% of the corresponding placebo group). In other studies, the best response was again seen in the crown and the least in the frontal area. Dutasteride, a dual inhibitor of both type I and type II 5α-reductase, has also been demonstrated to be well tolerated and effective in improving hair growth for patients with MPB. Although data are sparse, menopausal status, circulating androgen concentrations, and hyperandrogen symptoms do not appear to predict females’ response to finasteride – a known teratogen that is contraindicated in pregnancy. Side effects in men are infrequent, affecting less than 2% of patients. Despite the fact that they are generally reversed after discontinuation of the drug and often resolve during continued treatment, on April 11, 2012, the FDA amended professional labels for finasteride to reflect the reported continuation of erectile dysfunction, ejaculation disorders, and decreased libido after discontinuation of the drug. A 7-year clinical trial demonstrated a 24.8% reduction in the overall incidence of prostate cancer in patients on finasteride versus the placebo. Subsequent analyses revealed finasteride-related risk reductions of 30% for prostate cancer in general and 27% for high-grade prostate cancer, as well as suggesting increased prostate biopsy sensitivity with finasteride use. Although there is a dearth of well-controlled clinical trials involving other anti-androgens, such as spironolactone and cyproterone acetate, in women, it appears that the value of these medications is most pronounced in those with hyperandrogenism. Fortunately, for many patients with MBP and FPHL who are refractory to medical therapy, advances in surgical techniques make hair transplantation a reliably effective option (as seen in the accompanying figure of a 26-year-old with MPB (A) before and (B) 1 year after a 2649-follicular unit transplantation). The perfecting and worldwide adoption of ‘follicular unit transplantation’ (FUT) has yielded natural-appearing results combined with cosmetically good hair density per session, that was not possible until approximately 7 to 10 years ago. Improvements in the surgical approach now allow many female patients, as well as men in the early stages of MPB, to benefit from this procedure. Furthermore, ‘pluggy’ transplants that resulted from older forms of transplantation can now often be ‘retrofitted’ to make them appear natural, and areas of cicatricial alopecia secondary to disease, trauma, or cosmetic surgery can also be considerably improved. In addition, cosmetic aids can improve the appearance of patients with hair loss if medical treatments are either ineffective, not indicated, or if they are simply preferred as an adjuvant by the patient. Thinning hair can be camouflaged by coloring the scalp with tinted powders or sprays, as well as by the wearing of wigs and hair pieces. On the other hand, hair ‘extension,’ in which bunches of hairs are attached to individual scalp hairs, is generally discouraged owing to the potential for the development of permanent scarring traction alopecia. Only gold members can continue reading. Log In or Register to continue Related Related posts: Discoid lupus erythematosus Mucoceles Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Stay updated, free articles. Join our Telegram channel Join