Human skulls (Tenchini’s Collection, nineteenth century, courtesy of BIOMED—UNIPR, Parma, Italy). Schematics of the topography of the sensory (blue, dark yellow, red, magenta) and motor (green) innervation of the scalp in relation to the bones of the face and cranial vault. Each line represents a group of nerve fibers roughly distributing around its direction, whose (a–c) V1 ophthalmic, V2 maxillary, V3 mandibular branches of the trigeminal nerve (V), VII branches of the facial nerve, and C2–C3 branches of the cervical plexus. The topography of the sensory nerve axes of the scalp depicts a distribution coincidental with that of the arterial, venous, and lymphatic axes
2.2 Anatomy of Arteries, Veins, and Lymphatics of the Human Scalp
2.2.1 Arteries
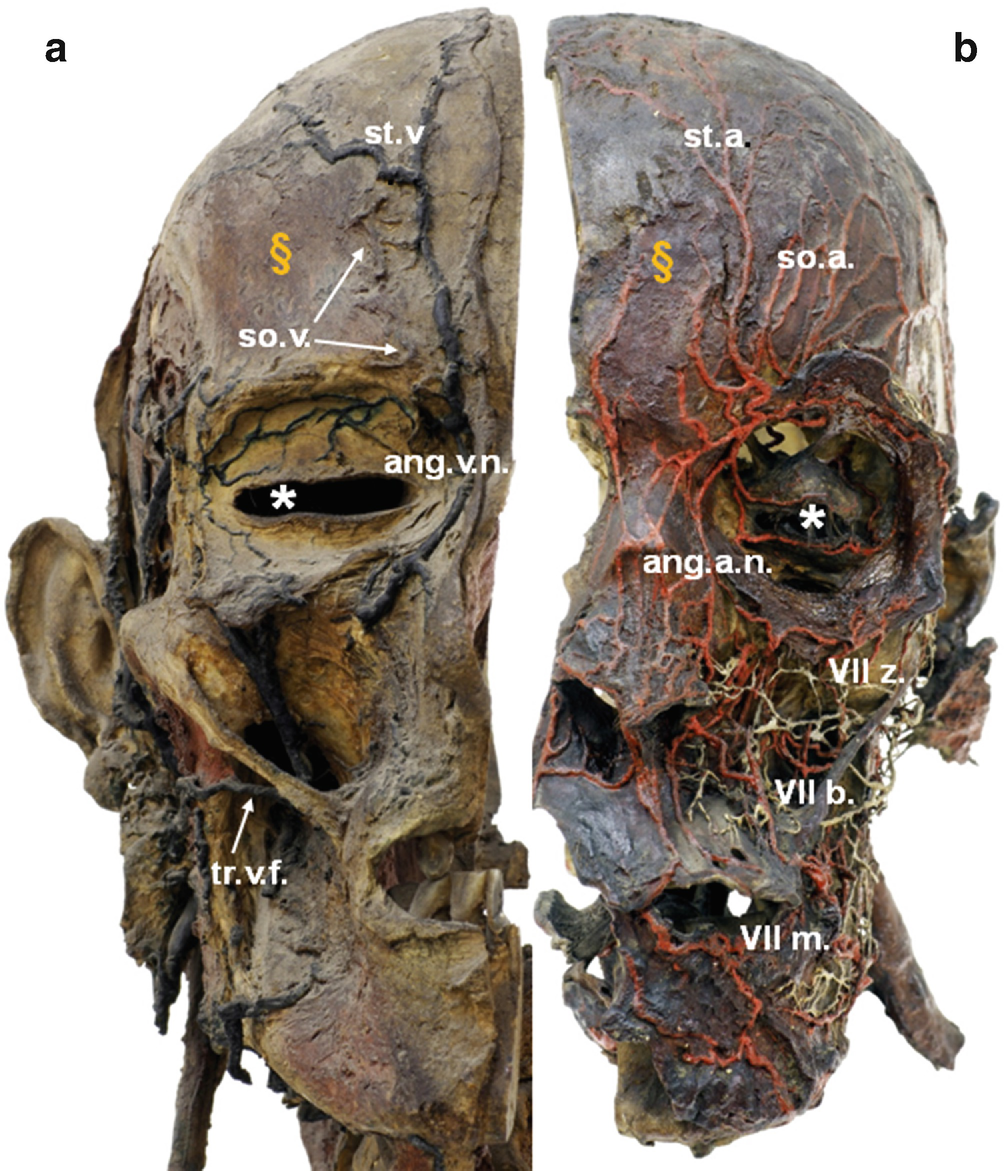
Montage of two midsagittal and symmetrical, dehydrated, and mass-injected halves of the adult male human head. Anterior view (Tenchini’s Collection, nineteenth century, courtesy of BIOMED—UNIPR, Parma, Italy). (a, b) ang.a.f. angular artery of the face, ang.v.f. angular vein of the face, so.a. supraorbital artery, so.v. supraorbital vein, st.a. supratrochlear artery, st.v. supratrochlear vein, tr.v.f. transverse vein of the face, white asterisk orbital cavity, § frontal belly of the epicranius muscle, VIIz zygomatic branch, VIIb buccal branch, VIIm mandibular branch of the facial nerve (VII)
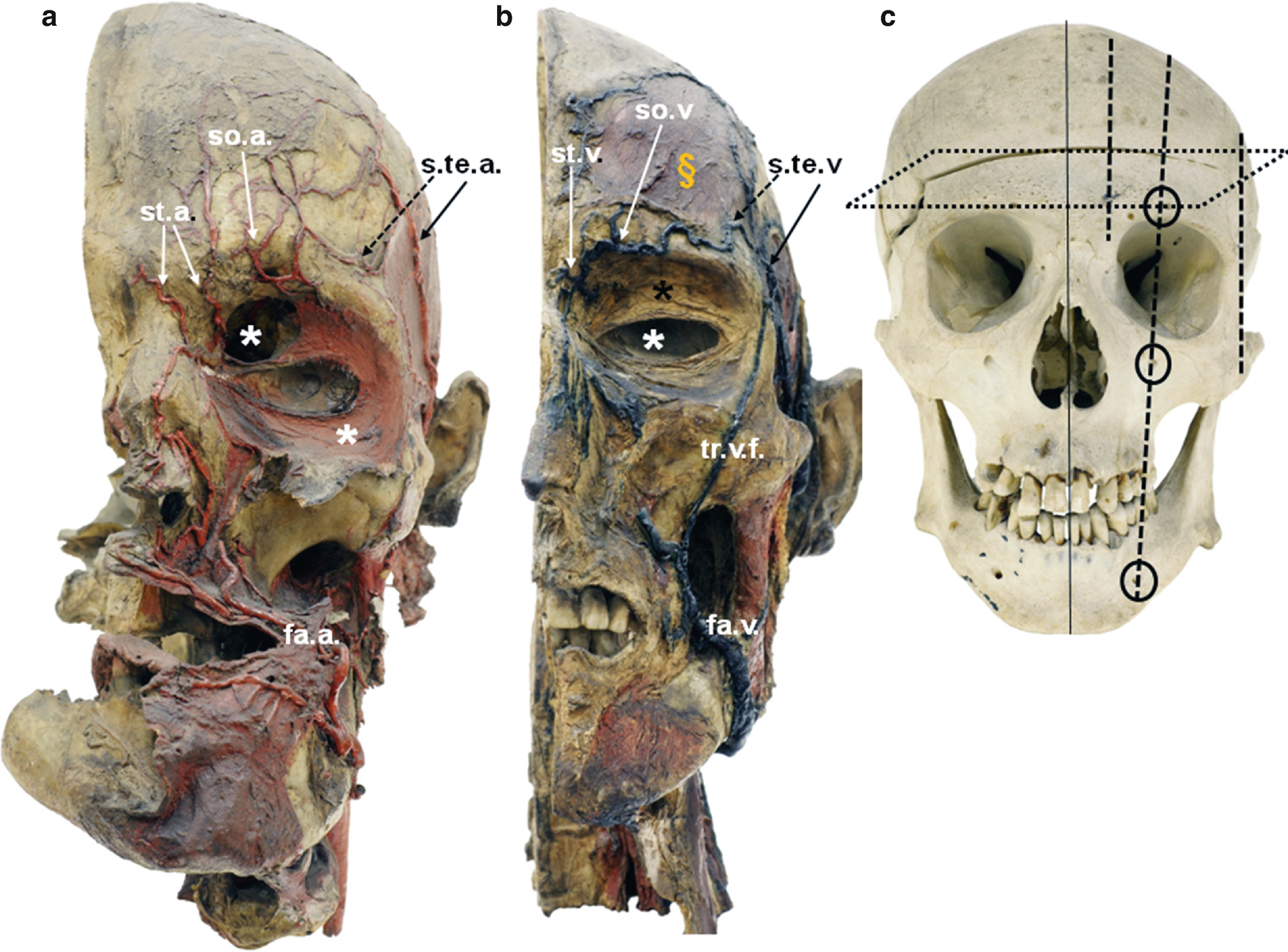
Dehydrated and mass-injected preparations of midsagittal halves of the adult male human head and entire skull. Anterior view (Tenchini’s Collection, nineteenth century, courtesy of BIOMED—UNIPR, Parma, Italy). (a, b): fa.a. facial artery, fa.v. facial vein, s.te.a. superficial temporal artery (dotted arrows depict frontal branches), s.te.v. superficial temporal vein (dotted arrows depict frontal branches), so.a. supraorbital artery, so.v. supraorbital vein, st.a. supratrochlear artery, st.v. supratrochlear vein, tr.v.f. transverse vein of the face, black asterisk orbicular muscle. In (a) the orbicular muscle is tilted downward with respect to its natural position, as in (b); white asterisk orbital cavity; § frontal belly of the epicranius muscle; (c) right to the midsagittal line: topography of the course of the arteriovenous axes of the calvaria. From medial to lateral, the vessels (above and below the ideal plane of dissection of the scalp from the facial bones) are distributed following three parallel lines, whose intermediate corresponds to that of vessels emerging from the three main facial foramina (circles supraorbital, infraorbital, mental). Note that the caudal to cranial direction of the vessels (and nerves as well, see Fig. 2.1) implies that surgical pedicle flaps of the scalp have to maintain a caudal continuity of these neurovascular axes to avoid inadequate healing/necrosis
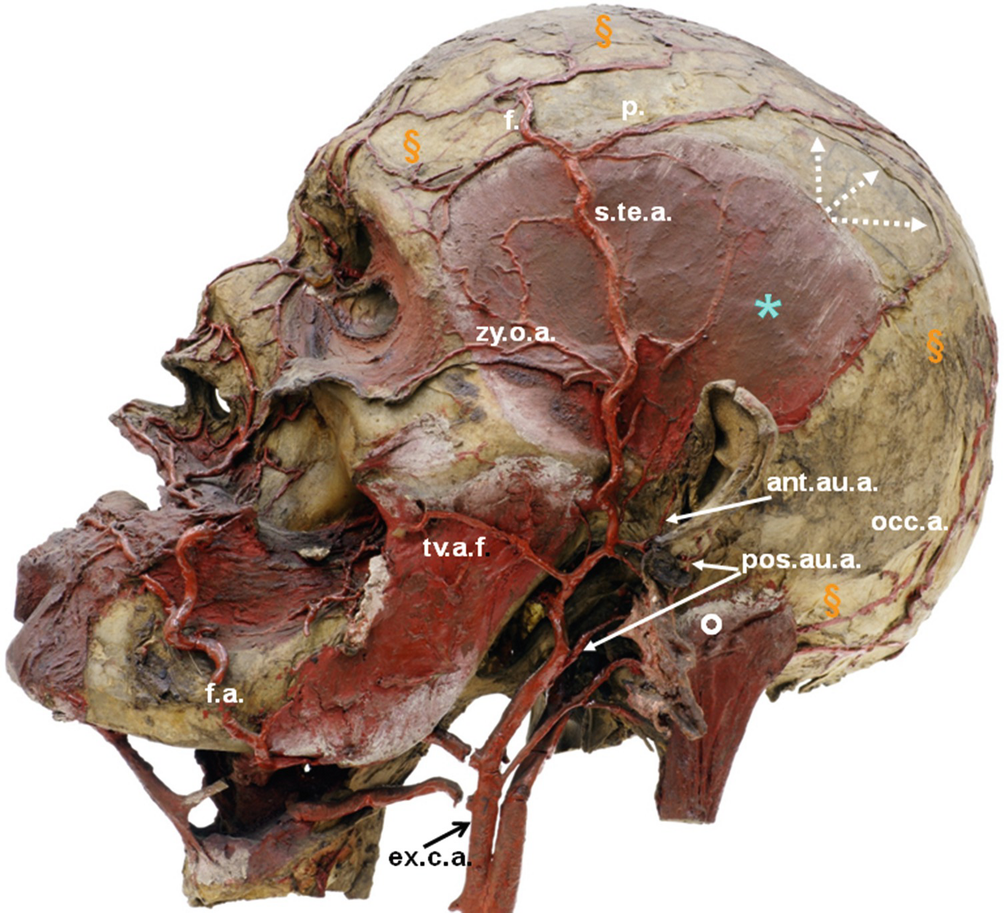
Midsagittal dehydrated and mass-injected half of the adult male, human head. Lateral view (Tenchini’s Collection, nineteenth century, courtesy of BIOMED—UNIPR, Parma, Italy). ant.au.a. anterior auricular artery, ex.c.a. external carotid artery, f.a. facial artery, occ.a. occipital artery, pos.au.a. posterior auricular artery, s.te.a. superficial temporal artery (f frontal branch, p parietal branch), tv.a.f. transverse artery of the face, zy.o.a. zygomatico-orbital artery, light blue asterisk temporalis muscle, § aponeurosis epicranialis, white circle occipital belly of the epicranius muscle. Dotted arrows originate from the superior edge of the temporalis muscle at the level of attachment of its fascia (superior temporal line), lay onto the parietal pericranium exposed by removal of the epicranial aponeurosis, and point to the line of dissection of the galea capitis originally in continuity with the superficial layer of the temporal fascia. Due to this continuity, infections of the scalp can extend into the temporal fossa but cannot reach the neck due to fixation of the superficial layer of the temporal fascia to the zygomatic arch
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
 Modification of Site 4 Decompression: Endoscopic Assisted Decompression of the Greater Occipital Nerve (GON) with Radical Excision of the Occipital Artery
Modification of Site 4 Decompression: Endoscopic Assisted Decompression of the Greater Occipital Nerve (GON) with Radical Excision of the Occipital Artery
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


