6 Anatomy of the aging face
Synopsis







Introduction
Facial aging is a complex process that is the cumulative effect of simultaneous changes of the many components of the face as well as the interaction of these components with each other. An understanding of the anatomical changes associated with aging is required in order to design effective procedures to rejuvenate various aspects of the aging face. Fundamental to understanding these changes is a firm grounding in the principles on which the facial soft tissue layers are constructed.1 This is important because the pathogenesis of facial aging is explained on an anatomical basis, particularly the variations in the onset and outcome of aging seen in different individuals. Understanding the principles on which the facial soft tissues are constructed is the basis for an accurate and reliable intraoperative map for the surgeons to safely navigate to the area of interest to correct aging changes. This is most important in addressing the overriding concern, being the course of the facial nerve branches. An anatomical approach to surgical rejuvenation of the face provides the way to obtaining a “natural” result that is lasting and with minimal morbidity.
Regions of the face
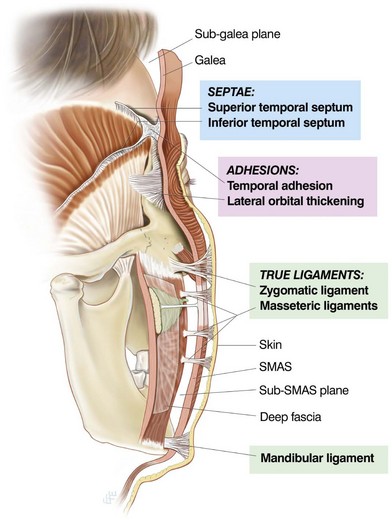
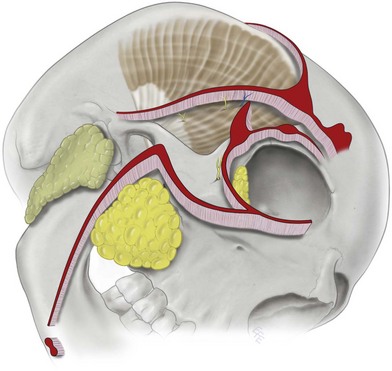
The traditional approach to assessing the face is to consider the face in thirds (upper, middle, and lower thirds).2 While useful, this approach limits conceptualization, as it is not based on the function of the face. From a functional perspective, the face has an anterior aspect and a lateral aspect. The anterior face is highly evolved beyond the basic survival needs, specifically, for communication and facial expression. In contrast, the lateral face predominantly covers the structures of mastication.3 A vertical line descending from the lateral orbital rim is the approximate division between the anterior and lateral zones of the face. Internally, a series of facial retaining ligaments are strategically located along this line to demarcate the anterior from the lateral face (Fig. 6.1). The mimetic muscles of the face are located in the superficial fascia of the anterior face, mostly around the eyes and the mouth. This highly mobile area of the face is designed to allow fine movement and is prone to develop laxity with aging. In contrast, the lateral face is relatively immobile as it overlies the structures to do with mastication, the temporalis, masseter, the parotid gland and its duct, all located deep to the deep fascia. The only superficial muscle in the lateral face is the platysma in the lower third, which extends to the level of the oral commissure.
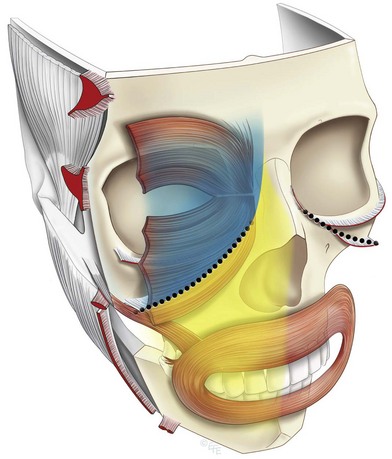
Importantly, the soft tissues of the anterior face are subdivided into two parts; that which overlies the skeleton and the larger part that comprises the highly specialized sphincters overlying the bony cavities.4 Where the soft tissues overlie the orbital and oral cavities they are modified, as there is no deep fascial layer for support. Accordingly, support does not come from within the cavity beneath, but from the rim of the cavities. The transitions between these areas, while not seen in youth, become increasingly evident with aging.
Surgical anatomy of the face, SMAS, facial spaces and retaining ligaments
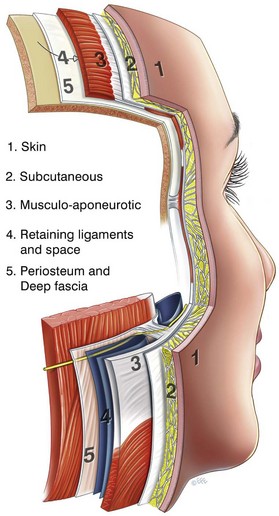
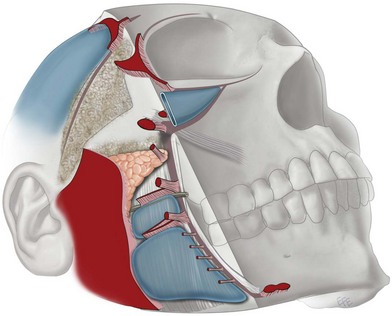
The soft tissue of the face is arranged concentrically into the five basic layers5,6: (1) skin; (2) subcutaneous; (3) musculo-aponeurotic layer; (4) areola tissue; and (5) deep fascia. This five-layered arrangement is most clearly seen in the scalp and forehead as a result of evolutionary expansion of the underlying cranial vault necessary to accommodate the highly developed frontal lobe in humans. Accordingly, the scalp is an excellent place to study the principles of the layered anatomy (Fig. 6.2). Layer 4 (the loose areolar tissue) is the layer that allows the superficial fascia (defined as the composite flap of layers 1 through 3) to glide over the deep fascia (layer 5). The simplified anatomy over the scalp gives the basic prototype of layer 4. There are not any structures crossing this plane, which is essentially an avascular potential space. At the boundaries of the scalp along the superior temporal line and across the supraorbital rim, the scalp and the forehead are firmly anchored by ligamentous attachments. Vital structures, the nerves and vessels are always located in close proximity to the retaining ligaments. In the face proper, while the principles of construction remain the same, there is considerably greater complexity. This is due to the compaction resulting from the absence of forward projection of the midface, as occurs in other species, and the predominance of the orbital and oral cavities that limit the availability of a bony platform for attachment of ligaments and muscles. To secure the superficial fascia to the facial skeleton, a system of retaining ligaments bind the dermis to the skeleton, and the components of this system pass through all layers (Figs 6.3, 6.4).7,8
The structure and composition of each of the 5 layers will now be described in turn.
Layer 2: subcutaneous tissue
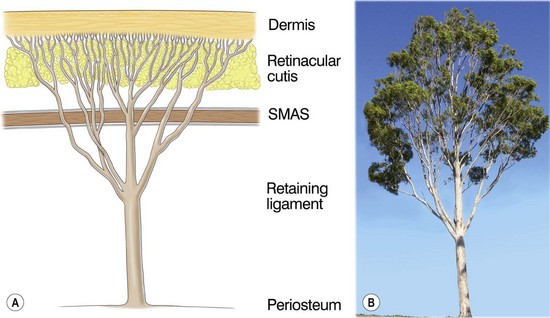
The subcutaneous layer has two components: the subcutaneous fat, which provides volume, and the fibrous retinacular cutis that binds the dermis to the underlying SMAS.9 Of note, the retinacular cutis is the name given to that portion of the retaining ligament that passes through the subcutaneous tissues. The amount, proportion and arrangement of each component vary in different regions of the face. In the scalp, the subcutaneous layer has uniform thickness and consistency of fixation to the overlying dermis. In contrast, in the face proper, the subcutaneous layer has significant variation in thickness and attachments. In specialized areas such as the eyelids and lips, this layer is significantly compacted such that fat may appear non-existent. In other areas, such as the nasolabial segment, it is very thick.4 In areas with thick subcutaneous tissue, the retinacular cutis lengthens significantly, predisposing its fibers to weakening and distension with aging. Within the subcutaneous tissue, the overall attachment to the overlying dermis is stronger and denser than the attachment to the underlying SMAS.9 This is a result of the tree-like arrangement of the retinacular cutis fibers (Fig. 6.3), with fewer but thicker fibers deep as its rises through the SMAS that progressively divide into multiple fine microligaments as they reach the dermis. This explains why it is easier to perform subcutaneous dissection in the deeper subcutaneous level (just on the surface of the underlying SMAS) than more superficially nearer the dermis, as there are fewer retinacular cutis fibers and the subcutaneous fat here does not attach directly to the outer surface of the underlying SMAS.
Furthermore, the retinacular cutis fibers are not uniform across the face, but vary in orientation and density according to the anatomy of the underlying deeper structures. As will be apparent when the anatomy of the underlying Layer 4 is described, at the location of the retaining ligaments, the vertically orientated retinacular cutis fibers are the most dense and are the most effective in supporting for the overlying soft tissues and in so doing, forms boundaries that compartmentalize the subcutaneous fat. These areas, such as the so-called McGregor’s patch over the body of the zygoma, often require sharp release to mobilize. In between these retaining ligaments in layer 4 are located the soft tissue spaces of the face, that facilitate the mobility of the superficial fascia over the deep fascia. Where the subcutaneous fat overlies a space, the retinacular fibers are less dense and orientated more horizontally, as a result of which, the tissues tend to separate with relative ease, often with just simple blunt finger dissection (Fig. 6.5). This variation in the density and orientation of the retinacular cutis fibers in the subcutaneous fat is the anatomical basis for the compartmentalization of the subcutaneous fat into discrete compartments, described in detail in Chapter 11.1.10,11
Layer 3: musculo-aponeurotic layer
The muscles of facial expression are unique and fundamentally different from skeletal muscles beneath the deep fascia because they are situated within the superficial fascia and they move the soft tissues of which they are a part. All muscles of facial expression have either all or the majority of their course within layer 3 and they are predominantly located over and around the orbital and oral cavities. In the prototype scalp, the occipital-frontalis moves the overlying soft tissue of the forehead, while its undersurface glides over the subaponeurotic space (layer 4). Layer 3 is continuous over the entire face, although for descriptive purposes, different names are given to certain parts according to the superficial muscle within. It is called the galea over the scalp, the temporoparietal (superficial temporal) fascia over the temple, the orbicularis fascia in the periorbital region, the superficial musculoaponeurotic system (SMAS) over the mid- and lower face and platysma in the neck.5,12
Layer 4
Layer 4 is the plane in which dissection is performed in subSMAS facelifts. It is an area of significant complexity and contains the following structures: (1) soft tissue spaces; (2) retaining ligaments; (3) deep layers of the intrinsic muscles passing from their bone attachment to their more superficial soft tissue origin; and (4) facial nerve branches, passing from deep to superficial. Functionally, a series of soft tissue spaces exist in layer 4 to allow independent movement of the periorbital and perioral muscle of facial expressions over the deep fascia responsible for mastication directly beneath the muscles of facial expression.13 The retaining ligaments of the face are strategically placed within the boundaries between the soft tissue spaces and functions to reinforce the boundaries (Fig. 6.6). In the lateral face, immediately in front of the ear, extending 25–30 mm forward of the ear cartilage to the posterior border of the platysma, is a diffuse area of ligamentous attachment, described by Furnas as the platysma auricular fascia (PAF).7 As no facial expression occurs here, the dermis, subcutaneous tissue, SMAS and the underlying parotid capsule (layers 1–5) are bound together as an area of retaining ligament. Layer 4 is reduced to a layer of fusion here, without a soft tissue space. The ligamentous character of this immobile area makes it surgically useful for suture fixation. Furnas had originally described the lower part of the PAF, the platysma auricular ligament,7 also named by Stuzin and colleagues, the parotid cutaneous ligament5 and this ligament was subsequently named the tympanoparotid fascia.14 The part of the PAF immediately in front of the lower tragus has been labeled, Lore’s fascia.14
Anatomy over the cavities in the skeleton
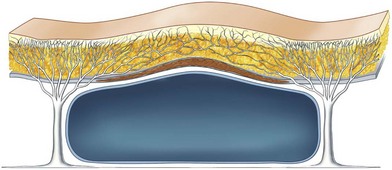
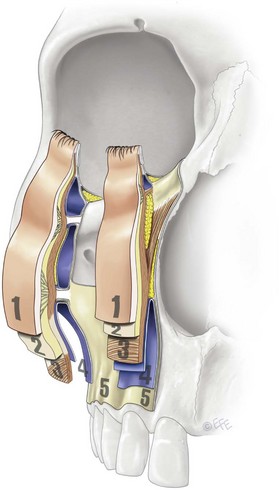
The general pattern of the five-layered anatomy is modified where the soft tissues overlie the orbital, oral and nasal cavities over the anterior face (Fig. 6.7). Only the outer three layers of the composite continue from the periphery as the soft tissue over the cavities. The SMAS layer within this composite includes the sphincteric orbicularis muscles that extend right to the free edge of the soft tissue aperture of the eyelids and lips. The retaining ligaments, which are such a key feature of the five-layered anatomy, are not present over the cavities. There are thus anatomical variations associate with thee functional transitions from the relative stability of the “fixed” areas to the high mobility of the soft tissue shutters over the cavities. At the transition, to support the shutters, the retaining ligaments are condensed along the bony orbital rim (Fig. 6.8). This is the anatomical basis for the periorbital ligament around the orbit, of which the lower lid part is the orbicularis retaining ligament, which stabilizes the orbicularis oculi to the orbital rim periosteum. Around the oral cavity where the boundary is less distinct, the ligaments arise mainly from the platform of the body of the zygoma, and from the deep fascia over the masseter.15–17
Facial spaces
A large part of the subSMAS layer 4 consists of soft tissue “spaces.” These spaces have defined boundaries that are strategically reinforced by retaining ligaments.18 Significantly, these areas are by definition anatomically “safe spaces” to dissect, as no structures crosses within and all branches of the facial nerve are outside these spaces. As the roof of each space is the least supported part, it is more prone to developing laxity with aging, compared with the ligament-reinforced boundaries. This differential laxity accounts for much of the characteristic changes that occur with aging of the face. Once a space has been surgically defined to its boundaries, the retaining ligaments in the boundary can then be precisely released under direct vision to achieve the desired mobilization, while preserving the vital structures closely associated with the ligaments. A brief description of surgically significant facial soft tissue spaces is given below.
Upper temporal space
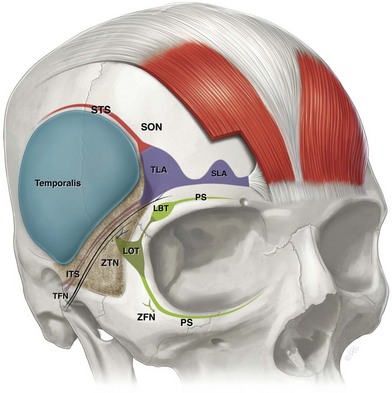
The upper temporal space separates the temporoparietal fascia (superficial temporal fascia) from the (deep) temporal fascia and is separated from the forehead by the superior temporal septum (STS) along the superior temporal line (Fig. 6.9). Anteroinferiorly, the upper temporal space is separated from the lower triangular shaped temporal area that contains important anatomy, by the inferior temporal septum (ITS). These septi merge at the triangular-shaped zone of adhesion called the temporal (orbital) ligament.15 The upper temporal space provides safe surgical access to the lateral brow and upper mid-cheek. The space can be readily opened by blunt dissection to its boundaries. Once identified, the boundaries are then released by precise sharp dissection. The superior temporal septum can be released sharply, taking care only to preserve the lateral (deep) branch of the supraorbital nerve, which runs parallel to the septum about 0.5 cm medial to it.19 The inferior temporal septum provides a marker to the important anatomy here as the temporal branches of the facial nerve are located parallel to and immediately inferior to this septum. To release the inferior temporal septum, the roof of the space is gently lifted off the deep temporal fascia floor, which three-dimensionalizes the septum in preparation for its gentle release at the level of the floor, bearing in mind the frontal branches are located under the roof of the lower temporal area where they travel in the ceiling within the layer of fat suspended on the underside of the temporoparietal fascia. Once released, the sentinel vein comes into view. The sentinel vein is not a good landmark for locating the temporal branches as they course cephalad to the vein, that is, inferior to the inferior temporal septum. This anatomy is also reviewed in Chapter 7.
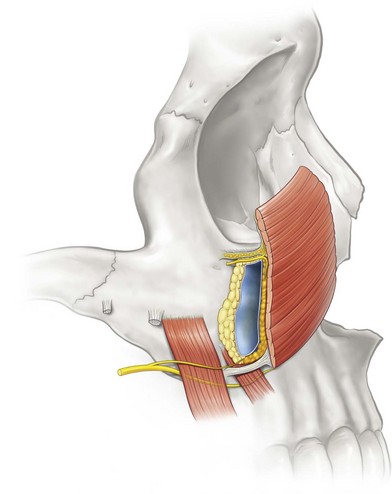
Prezygomatic space
This triangular-shaped space overlies the body of the zygoma, its floor covering the origins of the zygomatic muscles. The space allows the independent displacement of the orbicularis oculi (pars orbitale) in the roof from the zygomatic muscles under the floor. Contraction of the overlying orbicularis elevates the prezygomatic soft tissues, which results in zygomatic smile lines (below the crow’s feet) (Fig. 6.10). With the laxity of aging the roof of the space rests at a lower level than in youth. As a result, there is a now a greater amplitude of movement on orbicularis contraction that has the effect of exaggerating the zygomatic lines with aging.13,16 This aging of the prezygomatic space, with bulging over its roof accentuated by its well-supported boundaries, is the anatomical basis for the clinical entity variously described as malar mounds, bags or malar crescent. These deformities indicate the presence of significant laxity and the treatment is directed to tightening the laxity of the roof and upper ligamentous boundary.