Chapter 22 Anatomical Double-Bundle Anterior Cruciate Ligament Reconstruction Procedure Using the Semitendinosus and Gracilis Tendons
Introduction
The anterior cruciate ligament (ACL) is composed of the anteromedial bundle (AMB) and the posterolateral bundle (PLB), each with a different function.1–3 Since 2000, the author has reported the surgical principle4 and the latest procedure5 for an anatomical double-bundle ACL reconstruction that is intended to anatomically reconstruct the AMB and the PLB. In addition, the author’s team reported a prospective cohort study to evaluate this anatomical double-bundle procedure in comparison with single-bundle and nonanatomical double-bundle ACL reconstruction procedures using hamstring tendon grafts.6 Our procedure has several noteworthy characteristics. First, all four ends of two tendon grafts are grafted at the center of the anatomical attachment of the AMB or the PLB, not only on the femur but also on the tibia. Second, we use the transtibial tunnel technique to create femoral tunnels. Third, we use the hamstring tendon-hybrid graft,7,8 in which the femoral end is connected with an Endobutton CL and the tibial end is connected with a polyester tape. Fourth, we fix the polyester tape portion of the graft onto the tibia with two staples at 10 degrees of knee flexion, simultaneously applying a 30N load to each graft. In this chapter, the surgical principle and the procedure of our anatomical double-bundle ACL reconstruction are explained.
Procedure
Creation of Tibial Tunnels
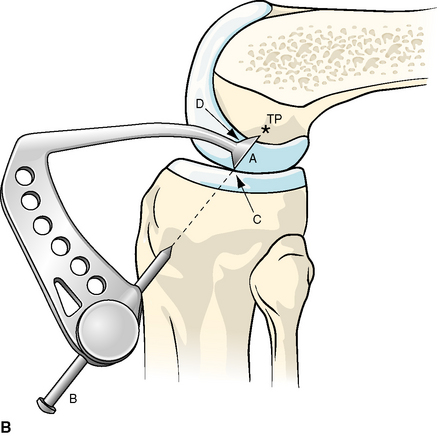
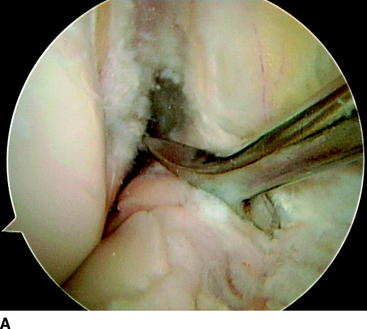
In ACL reconstruction procedures with the transtibial tunnel technique, the greatest key to success is to create a tibial tunnel with an appropriate three-dimensional (3D) direction. In other words, a tibial tunnel should be created so that a guidewire for femoral tunnel creation can be easily inserted at a targeted point on the lateral condyle through the tibial tunnel. To create such a tibial tunnel, we use a specially designed wire guide, called a wire navigator (Fig. 22-1, A), which was developed in our previous study.7,8 This device is composed of a navi-tip and a wire sleeve. The navi-tip consists of sharp tibial and femoral indicators. The axis of the wire sleeve passes through the tip of the tibial indicator (Fig. 22-1, B). First, a tibial tunnel for the PLB is created. The navi-tip is introduced into the joint cavity through the medial infrapatellar portal. The surgeon holds the tibia at 90 degrees of knee flexion, keeping the femur horizontal. The tibial indicator of the navi-tip is placed at the center of the PLB footprint on the tibia, which is located at the most posterior aspect of the area between the tibial eminences and 5 mm anterior to the posterior cruciate ligament (Fig. 22-2). Keeping the tibial indicator on this point, we aim the femoral indicator at the center of the PLB footprint on the femur (Fig. 22-3, A), which is precisely explained in the next section, and the proximal end of the extraarticularly located wire sleeve is fixed on the anteromedial aspect of the tibia through the skin incision made for the graft harvest. The proximal end and the direction of the wire sleeve are automatically determined depending on the direction of the intraarticular navi-tip (see Fig. 22-1, B). A Kirschner wire of 2 mm in diameter is drilled through the sleeve in the tibia. According to our basic studies, this tunnel does not injure this ligament because the insertion point of the wire on the anteromedial aspect of the tibia is located several millimeters anterior to the medial collateral ligament.4 The first tunnel is made with an approximately 6-mm cannulated drill corresponding to the measured diameter of the prepared substitute.

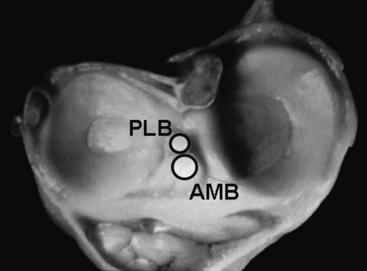

Next, a Kirschner wire for the AMB reconstruction is drilled using the same wire navigator. The tibial indicator is placed at the center of the tibial footprint of the AMB, which is located at a point approximately 7 mm anterior to the center of the first tunnel (see Fig. 22-2). Keeping the tibial indicator on this point, we then aim the femoral indicator at the center of the femoral footprint of the AMB (Fig. 22-3, B). The wire sleeve is fixed on the anteromedial cortex of the tibia. A Kirschner wire is then drilled through the sleeve in the tibia. The knee should be extended to ensure that the tip of the second wire is located at a point 5 mm posterior to the anterior edge of the roof in the intercondylar notch. The second tunnel is drilled with an approximately 7-mm cannulated drill corresponding to the measured diameter of the prepared substitute. Subsequently, two intraarticular outlets are aligned in the sagittal plane (see Fig. 22-2).
Creation of Femoral Tunnels
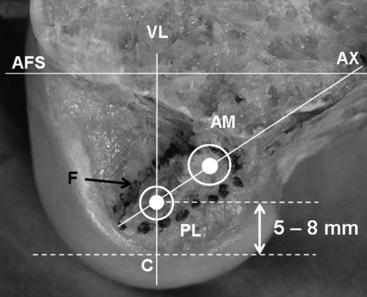
In the anatomical double-bundle procedure, it is essential to precisely understand the attachment of the main ACL fibers that should be reconstructed in ACL reconstruction. Although the normal ACL has a wide footprint on the lateral condyle,9–11 the author has found that the main ACL fiber attachment that should be reconstructed in ACL reconstruction is in the form of an egg, with its long axis inclined toward the posterior direction by 30 degrees to the long axis of the femur on the medial surface of the lateral femoral condyle4 (Fig. 22-4).
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 Arthrosis Following Anterior Cruciate Ligament Tear and Reconstruction
Arthrosis Following Anterior Cruciate Ligament Tear and Reconstruction
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


