Chapter 23 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts
A Four-Tunnel Technique
Introduction
Anterior cruciate ligament (ACL) reconstruction is now commonly performed, and the procedure has become progressively more reliable as our understanding of the ligament’s anatomy and biomechanics has improved. Correct tunnel placement, sturdy grafts, and rigid fixation techniques all contribute to a good postoperative outcome, but the contemporary literature reveals that success rates following single-bundle ACL reconstruction vary between 69% and 95%.1–3 Moreover, the persistence of a pivot “glide” (International Knee Documentation Committee Grade B) in 15% of cases4 has raised doubts as to whether subsequent arthrosis can be prevented. Single-bundle ACL reconstruction techniques do not completely reproduce the native anatomy and function. Grafts behave similarly to the anteromedial (AM) bundle of the ACL, resulting in anterior tibial translation not being fully controlled toward extension,5 where the posterolateral (PL) bundle has been shown to have a more important action. Several studies using different measurement techniques have also shown that single-bundle grafts are even less efficacious in providing rotatory stability.6–8
A number of authors have proposed reconstructing both AM and PL bundles to address these issues. Zaricznyj9 first published early clinical results of this type of procedure in 1987, but Japanese researchers were instrumental in subsequently developing “double-bundle reconstruction.” Combined with a strong European interest in the technique, several papers have since been published.10–27 These have described numerous technical variations using either one or two tibial or femoral tunnels, either autograft or allograft, and using different graft tensioning methods.
This chapter describes a double-bundle ACL reconstruction technique that uses two independent tibial and two independent femoral tunnels. This was first described by Franceschi et al16 in 2002 and subsequently refined.17,20
Surgical Procedure
Graft Harvesting
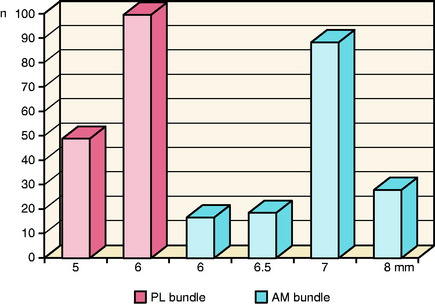
The gracilis and semitendinosus tendons are harvested using a tendon stripper as per a routine single-bundle hamstring reconstruction. The maximal length of tendon is harvested and the residual muscle removed. The gracilis graft (future PL bundle) is passed through a 15-mm continuous loop Endobutton-CL (Smith & Nephew, Mansfield, MA). A 20- to 30-mm Endobutton-CL is used for the semitendinosus graft (future AM bundle) due to the longer femoral AM tunnel. Each graft is then placed on a tensioning board and whipstitched with an absorbable #1 suture over 40 mm of its length. The two bundles are then calibrated. Grafts and the corresponding tunnel diameters are sized in 0.5-mm increments. The diameters of the double-stranded grafts are on average 6 mm for the PL bundle and 7 mm for the AM bundle (Fig. 23-1). If the diameter of the PL bundle graft measures less than 5 mm, we recommend attempting to triple the graft to increase its diameter. This is usually possible because the required length of the PL graft is shorter than the AM. If, however, the length is insufficient, then we recommend converting to a single-bundle technique.
Arthroscopic Reconstruction
The position of the arthroscopy portals is critical to allow the correct positioning of the bone tunnels. We recommend that the AM and anterolateral portals are made just adjacent to the corresponding borders of the patella tendon. Both should be placed as high as possible, just beneath the inferior border of the patella. The high anterolateral portal allows the tibial attachment of the ACL to be well visualized in the flexed knee. We do not find it necessary to use an accessory medial portal as proposed by Yagi et al.22 Following the arthroscopic evaluation and treatment of meniscal and articular lesions, the intercondylar notch is prepared. Scar tissue and ligament remnants are cleared from the 9 to 12 o’clock positions (the 12 to 3 o’clock positions in left knees), allowing the limits of the femoral ACL footprint to be well visualized.
Preparation of the Femoral Tunnels
The choice to drill the femoral tunnels via the AM portal and not via a transtibial approach is based on anatomical considerations. Several authors have shown that it is difficult to place a femoral tunnel in the anatomical attachment of the ACL via the transtibial approach.28–30 The advantages of using the AM portal have been outlined by Cha et al30 and Aglietti et al,21 who found that not only can the femoral tunnel be placed more anatomically, but that the femoral and tibial tunnels can be made independent of each other and that tunnel placement is also independent of graft type.
Although it is possible to drill the femoral AM tunnel via the tibial tunnel,24 it is not possible to reach the anatomical attachment of the PL bundle on the femur via this approach. In order to achieve anatomical placement of both tunnels on the femur, the alternative would be to use an “outside-in” approach.21,23 This necessitates the use of a second incision, made laterally, in order to position the drill guide. This approach is more invasive (incising both the lateral intermuscular septum and the capsule, which may be associated with some morbidity), and for this reason using the AM portal seems more appropriate.
After drilling the AM tunnel, a femoral PL bundle drill guide (Fig. 23-2) is used. The appropriate size guide is introduced into the AM tunnel and then rotated so that the PL bundle tunnel is positioned lower, more shallow, and more laterally (using notch navigation terminology) in the intercondylar notch at the 2:30 position (the 9:30 position in right knees). The drill guide allows the PL tunnel to be pierced with a 4.5-mm drill (again piercing the lateral cortex) so that the two femoral tunnels diverge at 15 degrees. With the knee flexed, the AM tunnel is more vertical, measuring 45 to 50 mm in length compared with the more oblique PL tunnel, which varies between 30 and 35 mm long. The PL tunnel should breach the cortex proximal to the tibial insertion of the lateral collateral ligament such that the cortical bone is sufficient to support the Endobutton. As with the AM bundle, the PL bundle is then dilated to the appropriate diameter. The drill guide is designed so that an approximate 2-mm bony bridge is left between the tunnels as they emerge into the intercondylar notch. This corresponds to the anatomical positions of the two tunnels in the femoral ACL attachment.
Related posts:
 The Central Quadriceps Free Tendon for Anterior Cruciate Ligament Reconstruction
The Central Quadriceps Free Tendon for Anterior Cruciate Ligament Reconstruction
 Proprioception and Anterior Cruciate Ligament Reconstruction
Proprioception and Anterior Cruciate Ligament Reconstruction
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


