CHAPTER 13 An Overview of the Modern Era of Breast Reduction
Key Terms
Reduction Mammaplasty
Goals of reduction mammaplasty
To best serve our patients’ needs and desires the surgeon needs a solid knowledge of anatomy.
Breast anatomy
Circulation
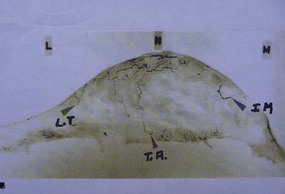
Maliniac1 in 1943 performed cadaver injections in 103 female breasts followed by roentgenographic studies. Mathes2 used latex and barium injections and dissections to further define the blood supply. His studies showed the main sources of blood supply to the breast (Fig. 13.1A, B) to be from:
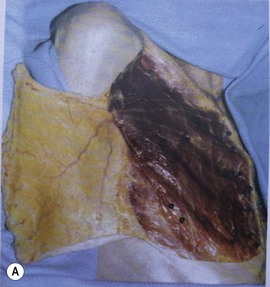
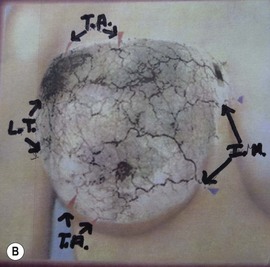
Fig. 13.1 An anatomic dissection performed by Dr. Stephen Mathes showing the vascular anatomy of the breast.
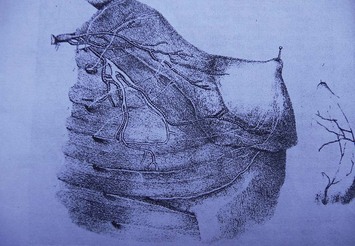
These studies, in addition, identify direct communications of the vascular network between the terminal branches of the lateral thoracic artery, the internal mammary artery, and the musculocutaneous branches of the thoracoacromial arteries and associated veins (Fig. 13.2).
Functional anatomy (lactation and innervation)
Before describing the various flaps we need to consider the pertinent anatomy of the breast parenchyma and the innervation of the nipple. The simplified version of breast parenchyma is that 10–100 alveoli comprise a breast lobule. Multiple lobules form a single lobe. Each lobe is drained by 15–20 lactiferous ducts. The end of a duct dilates becoming the lactiferous sinus which empties into the nipple. The nipple is composed of two layers of circular and longitudinal smooth muscle the contraction of which makes the nipple firm, erect and allows milk to be emptied from the lactiferous sinuses.4 The lobules are attached to the skin by dense fibrous bands termed Cooper’s ligaments. The breast is firmly fixed to the skin in the area of the areola.
Common sense tells us that there must be adequate parenchyma in the nipple bearing flap for sufficient milk production, and that the milk must have an intact pathway to the nipple which must be innervated so that it can become erect and empty on demand. It stands to reason that broader, thicker flaps will produce and transport more milk than narrower thin flaps. This is not to say that all or even most of the women undergoing reduction mammaplasty will want to be able to lactate postoperatively. It is however, the reason that surgeons whose primary technique greatly reduces or eliminates the possibility of breast feeding, should have the versatility required to employ a technique that retains normal breast function.6
Innervation
Nipple
Most authors agree that nipple sensibility is primarily derived from the lateral cutaneous branch of the fourth intercostal nerve3 (Fig. 13.3). Lesser contributions are made by the anterior cutaneous branches of the third, fourth, and fifth intercostal nerves and the third and fifth lateral cutaneous branches.
Skin
Innervation of the skin is not really a matter of practical concern in reduction mammaplasty because it comes superficially from all directions. The nerves are: (1) the supraclavicular branch of the cervical plexus from C3 and C4, (2) the lateral cutaneous branches of the anterior thoracic intercostal nerves, and (3) the anterior perforating cutaneous branches of the intercostal nerves.4,5,7
Fascia
The body’s superficial fascia system invests the breast parenchyma with a superficial and deep layer.7 The superficial layer has the same important role in reconstituting the breasts during reduction mammaplasty as does the superficial muscular aponeurotic system (SMAS) in the face and neck and Scarpa’s fascia in the abdomen during the rhytidectomy and abdominoplasty respectively. This superficial layer of fascia is immediately deep to the subcutaneous fat and needs to be incorporated in the medial and lateral limbs as it is the repair of this fascia that takes the tension off the skin closure, presumably resulting in a more favorable scar. Superficial fascia repair should be performed on all incisions except the periareolar which is repaired with deep dermal sutures.
The posterior layer of the superficial fascia is on the deep surface of the gland. Between it and the fascia of the pectoralis major muscle is the well defined retromammary space, which contains loose areolar tissue and allows the breast to glide freely over the chest wall.7
Skin marking patterns and scars
These basic configurations with multiple variations resulting in one or more of the following scars (Fig. 13.4A, B, C):
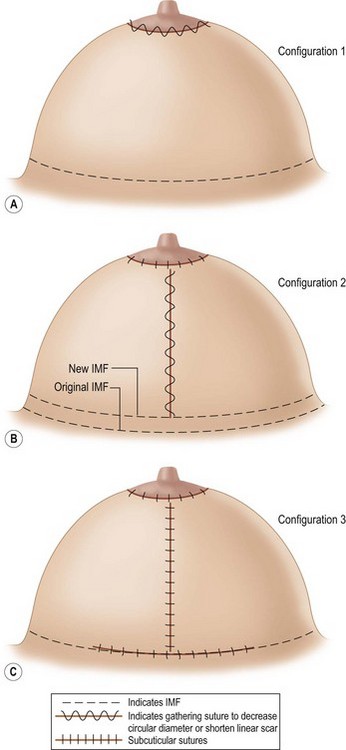
Analysis of Surgery Resulting in Configurations 1, 2, and 3
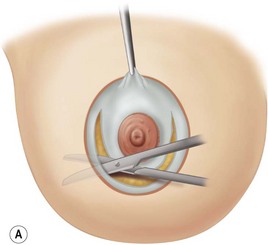
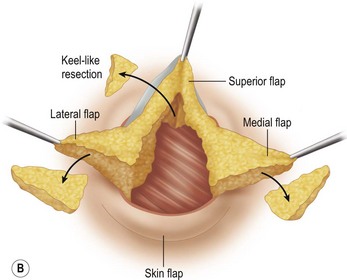
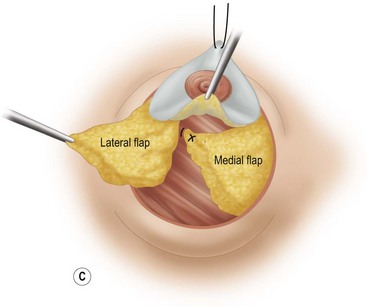
Configuration #18
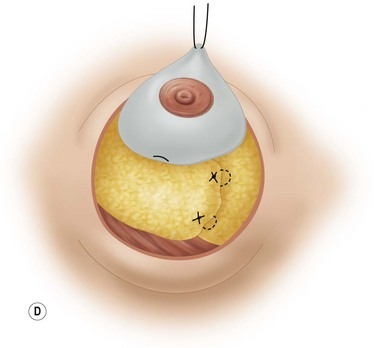
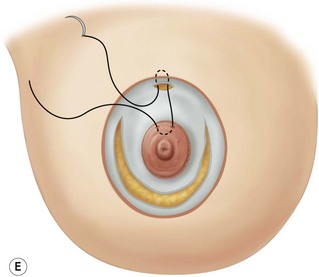
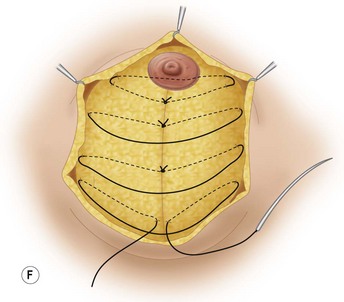
These diagrams demonstrate the oval skin and outer areola de-epithelialization pattern; the creation of a superior based flap with a crescent of parenchyma excised (Fig. 13.5A), the extent of which may be expanded to include tissue from the inferior, medial and lateral aspects of the breast (Fig. 13.5B). The medial and lateral glandular flaps are developed and crisscrossed under the superior based NAC flap (Fig. 13.5C, D). The superior (12 o’clock) aspect of the areola is then sutured in a subdermal window to the skin (gently folding the flap pedicle) and thus preventing enlargement of the scar (Fig. 13.5E) Lacing sutures traversing the entire thickness of the breast diameter support the conical shape of the breast and allows control of the NAC projection (Fig. 13.5F).
Disadvantages of the periareolar reduction mammaplasty are:
The proponents of this procedure have gained a degree of skill in this technique that the average plastic surgeon has found difficult to achieve. After an initial flurry of enthusiasm to utilize the periareolar procedure many have abandoned it. I am reluctant to criticize any technique that I have not tried to master. My initial bias against the technique was caused by the severe flattening created by the tension that the pursestring periareolar closure exerted on the breast mound. Benelli8 and Goes9 have overcome this by manipulating the breast mound with maneuvers such as crisscross flaps, lacing sutures, encompassing mesh, and extensive subcutaneous dissection to achieve aesthetically pleasing breasts. They appear to have succeeded by converting a compressible breast into a fixed, firm breast which resists the pressure of tight skin.
Configuration #2
Advocates of vertical mammaplasty use primarily the mosque shape or the open circle for the neonipple–areola site (Fig. 13.6D) The nipple site is centered to correspond to the meridian of the breast with the superior border of the areola located at the level of the IMF. The markings from the lower edge of the nipple–areola site make use of the meridian line as it projects on the upper abdominal wall and the breast is maneuvered medially and laterally to determine the edges of the medial and lateral limbs (Fig. 13.6A, B
Related posts:
 Gluteal Flap Breast Reconstruction
Gluteal Flap Breast Reconstruction
 The Central Septum in Breast Reduction and Mastopexy
The Central Septum in Breast Reduction and Mastopexy
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


