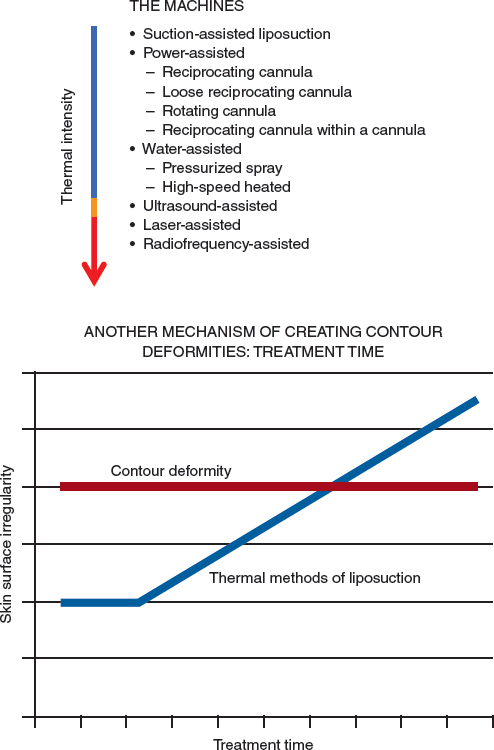
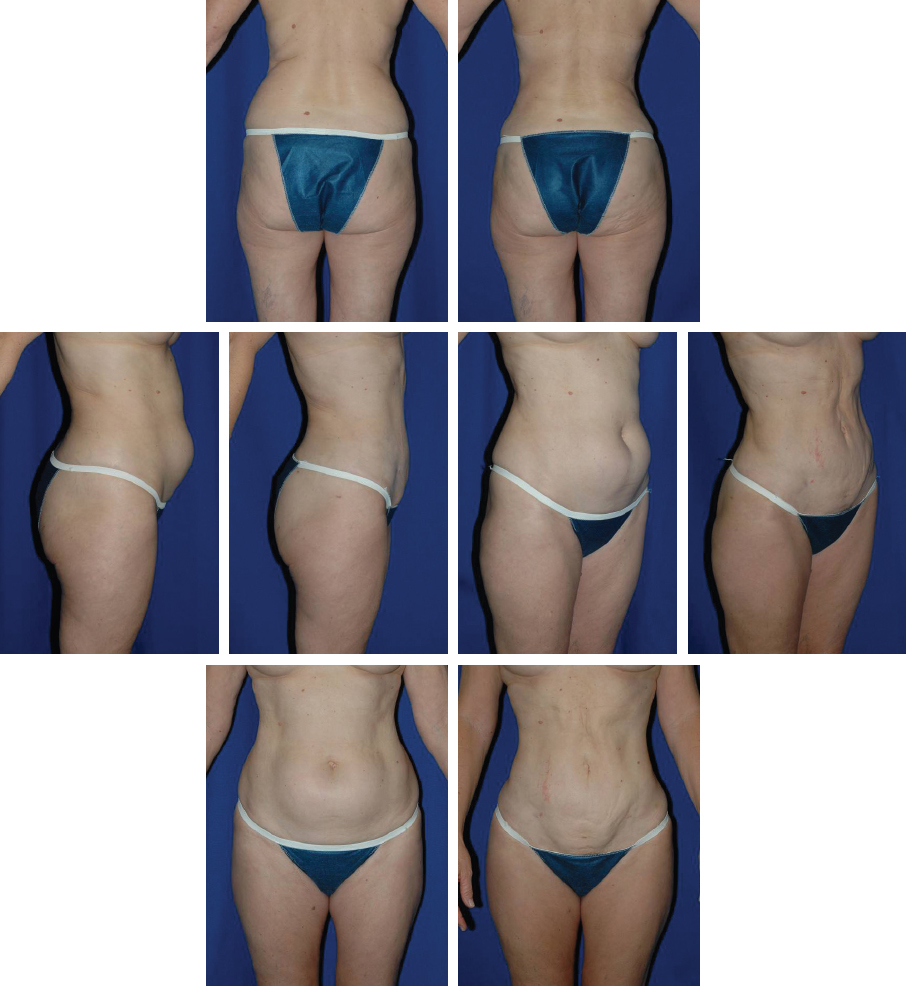
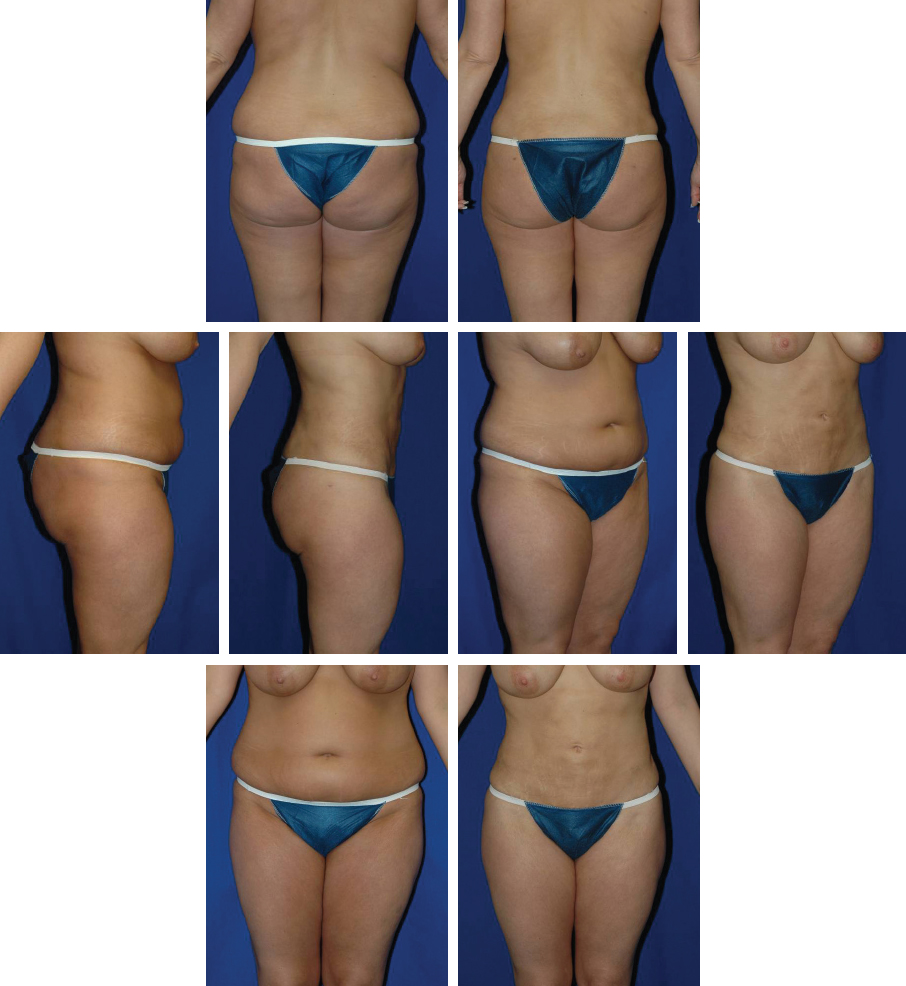
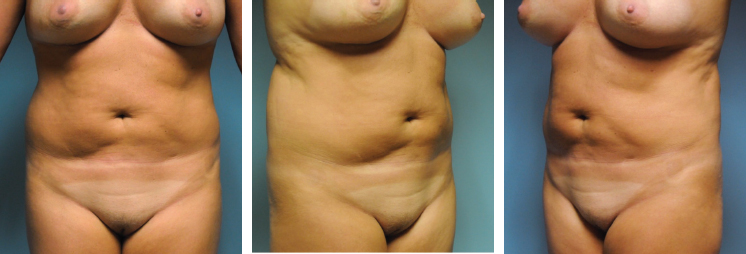
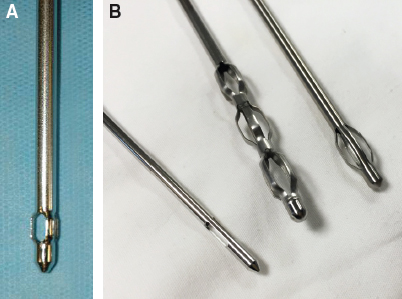
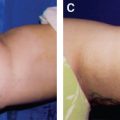
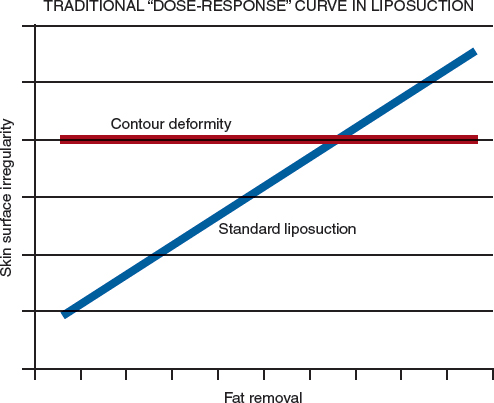
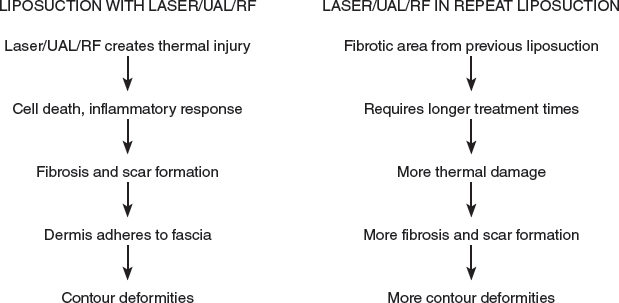
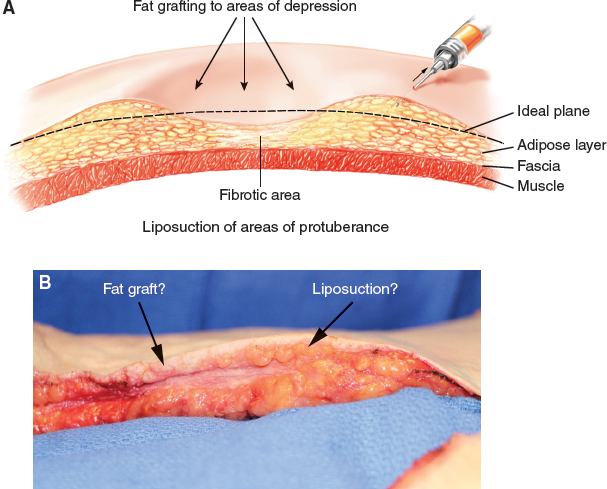
CHAPTER 15 Fig. 15-1 Despite more than 35 years of progress, including the ability to maintain patient safety in larger-volume liposuction procedures, no technique or technology to date has been able to break the dose-response curve* seen in liposuction, in which the dose is the increasing amount of fat removed from an area and the response is the tendency toward skin irregularities or contour deformities. Most well-trained and experienced surgeons have been able to work well within the boundaries that this dose-response curve dictates. Sometimes, however, the cosmetic results achieved fall short of patient and surgeon expectations, requiring secondary or even multiple additional procedures, none of which could ever match or exceed the result that could have been achieved in an optimal primary procedure. Many technologies have been advocated that purport to eliminate the uneven, irregular, wavy, or otherwise unsmooth appearance of the treated area where “too much fat was removed,” even though the amount of fat and skin pinch thickness were the amount desired by the patient and surgeon. Most of these proposed technologies use thermal energy—ultrasonic, laser, or radiofrequency. Not only have these technologies so far failed to reduce complications from liposuction, but also they have added an unintended, second dose-response curve, creating contour deformities based on the thermal load imparted to the tissues. Among other factors, such as the power, energy type, and how it is applied, the treatment time itself becomes the main contributor to creating contour deformities. It is for these reasons that I have abandoned the use of any internal thermal devices for fat reduction and instead use a comprehensive fat management process instituting fat separation, aspiration, and fat equalization (SAFELipo), which will be discussed extensively in this chapter. Revision liposuction and secondary liposuction procedures differ in a few important ways. Revision liposuction refers to a repeat operation usually performed by the same surgeon to improve the first result or to fix something left undone or not optimally performed during the first procedure. Secondary liposuction refers to procedures that are often, but not always, performed by a different surgeon, and are more extensive in nature than a revision procedure. Another distinction between revision and secondary liposuction is temporal: secondary procedures are usually not performed less than 1 year after the initial procedure, even if they are performed by the same surgeon. This chapter will mainly discuss secondary liposuction procedures, although much of the information will pertain to both revision and secondary liposuction, because both of these types of procedures are categorized as repeat procedures. Repeat procedures are performed for a variety of reasons, including unsatisfactory results or the need for further improvement. Frequently, a liposuction patient simply seeks further reduction to an area that was already treated, either because of weight gain or because he or she was dissatisfied with the amount or distribution of the liposuction. A typical candidate for a repeat procedure is a patient who underwent “spot” liposuction, usually of the upper or lower abdomen only. Because the entire abdominal or truncal unit was not contoured comprehensively, the patient is dissatisfied with the remaining area or areas of adiposity and therefore wants a more comprehensive procedure secondarily. More commonly, however, dissatisfied patients seek a secondary procedure to correct one or many contour deformities that resulted from an initial liposuction procedure. These contour deformities include overall skin waviness, hills and valleys, strange contours, and outright divots and depressions. In addition to these contour deformities, many patients have skin damage in the form of hemosiderin deposition, pigmentary changes, and scarring from thermal or avulsive liposuction methods. Internal scarring is seen as an unnatural static and/or dynamic appearance of the area, with tethering, tightness, and worsening appearance with positional changes or skin tension. External scarring is usually only seen with thermal methods of liposuction in which there were entry site burns, or even internal burns so severe that the overlying skin was burned and scarred. This 64-year-old woman underwent ultrasound-assisted liposuction (UAL) in which 3.7 L of fat was removed from the circumferential trunk. Note the uneven and irregular skin contraction of her abdominal skin. This 28-year-old woman underwent UAL in which 6.7 L of fat was removed from the circumferential trunk. Note the irregular appearance of the skin surface and stained appearance of the skin from hemosiderin deposition, which is commonly seen after thermal liposuction. This 38-year-old woman is shown 3 years after treatment elsewhere with a combination of UAL and laser-assisted liposuction (LAL) of the circumferential trunk. Note the severe skin irregularities with uneven skin retraction, deep and superficial contour deformities, and unnatural appearance of all of the treated areas. Fig. 15-7 This 24-year-old woman is shown 2 years after treatment with LAL to the medial and lateral thighs and buttocks. Note the irregular appearance of the skin surface, contour deformities, and asymmetrical collapse of the gluteal folds, giving an aged and unattractive appearance to the buttocks. This 35-year-old woman is shown before and 2 years after undergoing treatment elsewhere with LAL of the abdomen and flanks. Note the severe residual surface scarring, skin creases, uneven skin retraction, hemosiderin deposition, and contour deformities. Fig. 15-9 This 50-year-old woman was referred after having three previous liposuction surgeries of the circumferential trunk over a 5-year period: standard liposuction, UAL, and LAL. She also underwent multiple external radiofrequency treatments without improvement. Note the uneven skin contraction, deep contour deformities, areas of dense scarring, and overall skin surface irregularities. This 50-year-old woman was referred after receiving a single treatment of UAL with “abdominal etching.” Note the aged and cobblestone appearance of the abdominal skin, the unnatural appearance of the “etched” areas, and the overall poor contour. The feasibility of liposuction itself is based on the premise that there is a relatively low-resistance, “harvestable” subcutaneous adipose tissue layer between the higher-resistance planes of the overlying superficial fat and dermis above and the underlying musculoskeletal structures below. This differential in resistance between these planes is what allows a cannula to easily pass through and stay in the target fat layer. Thus liposuction works, because fat is less dense and easier to traverse, disrupt, and remove than the tissues that surround it. Once a liposuction procedure has been performed, this treatable tissue layer is scarred, adherent, or even obliterated, making navigation and fat extraction more difficult and potentially more dangerous, even for experienced surgeons. For example, in a primary liposuction procedure, significant resistance encountered at the cannula tip is generally a sign that the cannula should be redirected. In a revision or secondary procedure, this is not necessarily the case, so the surgeon must be able to discern whether the resistance is coming from a vital structure or from fibrotic subcutaneous tissue that remains from a previous procedure. This loss of differential resistance seen in repeat liposuction procedures is the main reason these procedures frequently result in problems, such as skin “end hits,” resulting from the natural tendency for the surgeon to redirect superficially, preferring to err here rather than in deeper structures. The loss of this low-resistance plane can also result in potentially fatal (and likely underreported) abdominal perforation or damage to other deeper structures. Despite these and other difficulties faced in repeat liposuction procedures, revision and secondary body contouring with liposuction can be very gratifying and successful for patients and their surgeons when the appropriate expectations, approach, care, and techniques are applied. I perform a somewhat “alternative” approach to the typical techniques that have been proposed for repeat liposuction. This technique can help many patients who otherwise have not previously had much hope of regaining a more normal or natural appearance. There are still liposuction patients with deformities from primary procedures who are not good candidates for repeat procedures; the majority of this subset of patients will have undergone thermal methods of liposuction. Repeat procedures are also associated with complications that are different from those commonly seen after primary liposuction procedures. I have compared performing repeat liposuction to operating in concrete. In repeat procedures, the differential in resistance between the intended and unintended planes is narrowed, sometimes even eliminated. As outlined previously, this difficulty in navigating through scarred, adherent subcutaneous tissues increases the risk of damage to the skin and deeper structures, resulting in a potentially life-threatening complication. These procedures also take more time to perform, which is another factor that increases overall risk. Obviously, in such an environment, fat extraction is more challenging, and smoothness and uniformity are more difficult to achieve. Cannula “misadventures”—injury to skin and body structure, vascular disruption and major bleeding, nerve damage, musculoskeletal injury, and internal organ perforation—have all been reported. Although these injuries are possible with any liposuction procedure, they are more likely to occur in repeat liposuction, in which there is a high-resistance, scarred, and confluent tissue bed that requires more cannula passes with greater force to adequately perform the procedure. It has also been stated that penetrating injuries from liposuction procedures are significantly underreported in the literature. Fig. 15-11 For these reasons, I have abandoned internal thermal technologies and use only fat-preserving techniques and technologies for both primary and repeat liposuction cases. Fat grafting and fat equalization are also an integral part of all of my contouring cases, necessitating a healthy recipient bed and healthy fat for maximum survival and regenerative potential. Many patients request repeat procedures for further fat reduction either because of underextraction during the initial procedure or reaccumulation of adiposity from weight gain. In these patients, it is easy to think that simply removing additional fat from the target areas is all that is required, again referred to as spot liposuction. In practice, however, even the “straightforward” repeat liposuction patient can be deceptively difficult to re-treat with liposuction because of the scar tissue and fibrosis encountered in nearly all of these cases. At best, these patients have a denser, more fibrous area in which to perform repeat liposuction, making it more difficult to extract more fat evenly. More commonly, these patients have fibrotic deep fat compartments that are mostly devoid of suctionable fat, with only a relatively superficial zone of fat to be navigated, having a variable amount of fibrosis and tethering to the overlying dermis and underlying fascia. For this reason, no repeat liposuction patient should be approached as a simple case. Fig. 15-12, A and B This illustration shows the traditional “spot approach” of either liposuction or fat grafting of individual areas, or “spots” (A). The cross-section of an actual patient with contour deformities shows the difficulty of using the “spot approach” in practice (B). An ideal body contouring procedure should be comprehensive in nature, with applicability in most or all situations. For most patients, this requires not just the removal of fat tissue, but also fat grafting and fat redistribution. The SAFELipo technique was developed specifically for repeat liposuction cases, in which fat grafting is often required, and the previously mentioned issues (that is, scarring, existing contour irregularities, and so on) often exist. SAFELipo is a multistep process of comprehensive fat management that not only reduces fat through liposuction, but also can augment and redistribute fat. There are other techniques used in repeat procedures. However, I use SAFELipo exclusively for both primary and secondary liposuction on all parts of the body and face. There will inevitably be a significant amount of overlap in how these techniques are used in primary versus secondary procedures, but my discussion focuses on how SAFELipo is employed in repeat procedures. SAFELipo differentiates itself from other forms of advanced liposuction techniques in a few important ways that will become apparent as the individual steps are explained. SAFELipo incorporates a process approach to fat contouring, with specific, repeatable delineated steps that standardize and simplify surgeries. A similar process approach has been applied to other cosmetic surgical procedures (for example, breast augmentation) and has been shown to be beneficial. And in contrast to thermal and avulsive forms of liposuction (standard suction-assisted liposuction [SAL]), SAFELipo greatly reduces the risk of disrupting blood vessels and supporting structures while maximizing the potential for an aesthetically pleasing outcome. Another differentiator with SAFELipo is that avoiding the zones of adherence and areas devoid of excess fat is unnecessary, in contrast to other forms of liposuction. Typically, contour deformities are caused by avulsing (aspirating) too much fat or the wrong layers of fat from an area, a problem compounded by areas that have minimal amounts of fat or areas that are more fibrous. Because there is no aspiration when performing fat separation and fat equalization, areas that are typically prone to contour deformities using standard liposuction techniques can be traversed without fear of oversuctioning or damaging them using SAFELipo. During the fat separation and equalization stages, the zones can be navigated, so the only time to be wary of these zones is when performing fat aspiration. SAFELipo allows a much more comprehensive treatment of entire anatomic areas given its ability to pass into any thin areas and zones of adherence without creating suction avulsion injuries. Good candidates for repeat liposuction generally have a BMI of 30 or below, good diet and exercise habits, and reasonable expectations regarding outcomes. For a patient who requests a secondary liposuction procedure to address reaccumulation of fat, all of these factors become even more important. On the other hand, a patient who was not adherent to postoperative care after their first procedure or who quickly gained weight after a previous body contouring procedure might be considered a suboptimal candidate for a repeat procedure. Because a patient requesting a repeat procedure has already had a bad experience, it is important that the surgeon carefully explain what to expect from a repeat procedure. Obviously, if the surgeon is not able to completely fix what is not aesthetically pleasing, he or she should explain that to the patient before a second or third procedure is performed. Also, it is important to make certain that the patient understands the limitations inherent in repeat procedures, as well as the likelihood that the result will not be as optimal as what could have been obtained with a better-performed first procedure. This is particularly true if the initial procedure involved the use of thermal liposuction because of the excessive amounts of scarring and fibrosis seen in these cases. In some cases, when patients have undergone one or more procedures using internal LAL, they cannot make significant improvements, so these patients should be advised to avoid undergoing another procedure. If the patient’s expectations are not likely to be met by any available techniques, or if the amount of surgery required becomes excessive to gain only a modest improvement, no operative plan will ultimately please the patient. Using an approach similar to performing revision rhinoplasty, I wait at least 1 year before performing a secondary liposuction procedure. That time is needed to ensure that all swelling has resolved and that the tissues are as pliable, soft, and elastic as possible. Additionally, because of the frequent need to add, redistribute, and subtract from an area, a stable and unchanging tissue bed is required before planning a reoperation. Most patients with moderate to severe contour deformities need 18 months to 2 years for swelling and tissues to settle before attempting a significant repeat liposuction operation, and the longer the time interval between the original surgery and the repeat operation, the higher the chances for long-term improvement and success. After their initial procedure or procedures, some patients are left with such a small amount of subcutaneous fat that it is impossible to perform a repeat procedure. Even with the SAFELipo process, there needs to be some amount of residual fat to create a smooth and natural-appearing contour. Cases that rely on pure fat grafting to create a smooth appearance are very difficult to execute and should be approached with extreme caution; perhaps they should not be performed at all. As with primary liposuction, intermittent or sequential compression devices on the lower extremities are applied before the induction of anesthesia and are used throughout the surgery and for several days postoperatively, or until the patient is ambulating normally. Passive and active patient warming maneuvers are employed from 1 hour before surgery until the patient is discharged from recovery to prevent hypothermia. Hypothermia, or a core temperature drop to below 36° C at any time during surgery, has been shown to increase bleeding, postoperative nausea and vomiting, and wound infection. Anecdotally, I have also seen more difficulty in postoperative pain management in patients who became hypothermic during surgery. Forced air units, heat-retaining stockinettes, circulating hot-water mattresses, intravenous fluid warmers, warm infiltration fluids, warm prep solution, and a warm (74° F) room during prepping are all used in significant primary or repeat body contouring procedures. In contrast to the single-colored topographic markings made in most primary liposuction cases, repeat liposuction procedures usually require more distinct topographic markings to clearly delineate the hills and valleys. Although a spot approach to correcting these cases is not used, it is still wise to have a relatively detailed map of the areas to be reduced, redistributed, or augmented; these areas are usually represented by concentric black rings for reduction and crosshatched markings in red for areas of redistribution or augmentation. It has also been useful to make orientation marks on the treated areas to aid in symmetry while treating in various body positions. Repeat liposuction procedures are typically performed with the use of a general anesthetic. Except for minor touchup procedures, repeat liposuction procedures do not lend themselves to being performed under local, tumescent, or conscious sedation anesthesia for the same reasons that these methods are not used for significant primary liposuction procedures. Additionally, the dense scar tissue and unnavigable tissue planes that are frequently encountered limit the surgeon’s ability to easily, completely, or painlessly pass infiltration, separation, or liposuction instruments. The positioning for repeat liposuction does not inherently differ from that of primary liposuction. That said, whenever possible, I avoid having the patient in the prone position. Adequate padding of all pressure points is important, including those involved in any positional changes, along with careful sterile prepping and draping. I prefer to do a single whole-body prep, with the sterile field extending from the neck down to the end of the bed so that the patient can be moved into different positions during the procedure without the need for further prepping. Revision liposuction using the SAFELipo process is typically performed in three positions: supine, and both the left and right lateral decubitus positions. Although evidence is currently lacking, turning the patient multiple times, including into the lateral decubitus position, may reduce the risk of deep vein thrombosis and pulmonary embolism, because venous pressure is decreased on the elevated side, decreasing pooling and improving pelvic venous drainage. SAFELipo is a multistep body contouring process that offers a comprehensive fat management solution. The application of a process approach to either primary or repeat liposuction simplifies the technique on many levels, and allows a much more complete treatment of the targeted areas, whether they require the removal, redistribution, or addition of fat. Compared with other methods of liposuction, SAFELipo enables the smooth removal of any or all excess fat from the targeted areas without fear of causing skin injury or contour deformity. As previously mentioned, SAFE is an acronym for separation, aspiration, and fat equalization. These are the steps taken in primary liposuction cases. In secondary cases, a fourth step is frequently added that can include fat shifting, grafting, and release processes to attend to any residual defects or volume deficiencies. In any liposuction procedure, adequate infusion of the wetting solution is crucial to minimizing blood loss, providing additional anesthesia, and increasing working space through volume expansion. In primary cases, a typical superwet infusion is used, with an infusion-to-aspiration ratio of 1:1 or 1.5:1. In a repeat procedure, in which volume expansion of the target zone is even more vital to being able to adequately traverse the tissue planes, a tumescent approach with a ratio of 2:1 or even 3:1 is frequently needed. In the past, a Klein needle was used for this important aspect of the procedure, encompassing an infusion phase and then roughly 20 minutes of waiting to allow maximum vasoconstriction of the tissues before performing step 1 of the SAFELipo process, separation. In the course of applying SAFELipo concepts to his liposuction and fat grafting procedures, Dr. Daniel Del Vecchio first proposed the utility of performing simultaneous separation and tumescence. The time needed for maximum vasoconstriction to take effect is drastically reduced by simultaneously infiltrating the wetting solution while performing step 1, separation.
Alternative Approach to Repeat Liposuction
Definitions
Reasons for a Repeat Procedure


Difficulties Inherent in Repeat (Revision or Secondary) Liposuction
Indications and Contraindications
Patient Evaluation
CLINICAL EVALUATION OF THE DEFORMITY
Preoperative Planning and Preparation
Surgical Technique
MARKINGS
ANESTHESIA
PATIENT POSITIONING
TECHNIQUE
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine