CHAPTER 20 Alloplastic Contouring for Suborbital, Maxillary, Zygomatic Deficiencies
Alloplastic facial contouring has evolved from being an ‘ancillary procedure’ to a standard valuable tool in the armamentarium of aesthetic facial surgeons over the last 25 years. This author has pioneered most of the implants and techniques now used by surgeons worldwide.1 These have proven over time to create contour corrections of permanence and with minimum (less than 1%) morbidity. The many myths about alloplastic augmentation have been dispelled by the author from his 30 years of experience confirming that these techniques can now be used safely and effectively by any well-trained plastic surgeon who has an interest in 3-dimensional aspects of aesthetic facial surgery.
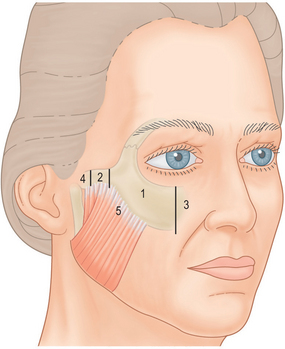
According to my original anatomic zonal concepts of the facial skeleton (Fig. 20-1) the suborbital zygomatic region is comprised of: (1) Zone 1, the major body of the malar bone defined medially from the infraorbital nerve and laterally by the beginning of the middle third of the zygomatic arch and (2) Zone 3, the paranasal suborbital zone which extends from the nasal bone – maxillary tissue to the infraorbital nerve. This zone contains the well-described ‘tear trough’ sulcus.
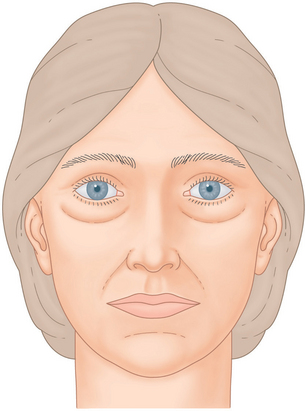
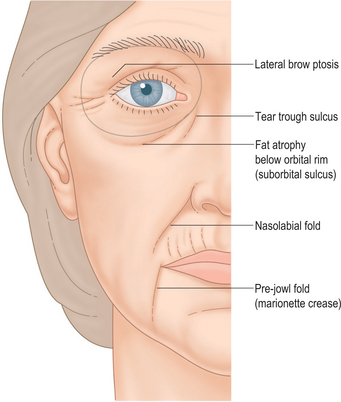
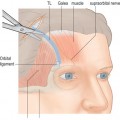
The suborbital region has commanded significant attention over the past 10 years due to the advent of upper midface suspension techniques designed to improve a tired, hollow appearance from the depression of the lid-cheek junction2,3 (Fig. 20-2) which occurs mostly with the aging process but also as a hereditary variant. Moreover, it has now been validly established by prominent investigators that the aging process of the upper midface results largely from atrophy or shrinkage of the volume of fat contained in the periorbital and malar region that is present in the youthful phases of life, birth to age 30 on the average4,5 (Fig. 20-3).
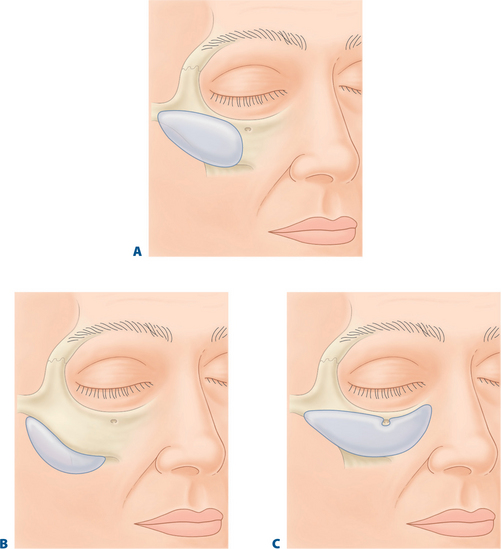
Alloplastic implants designed specifically for the suborbital tear trough malar region can eliminate the need for techniques using fat rearrangement in the inferior orbital and suborbital region (Fig. 20-4). These fat manipulations may produce undesired sequelae such as lower lid retraction (ectropion) and visible unattractive irregular ‘lumpiness.’
Historical background
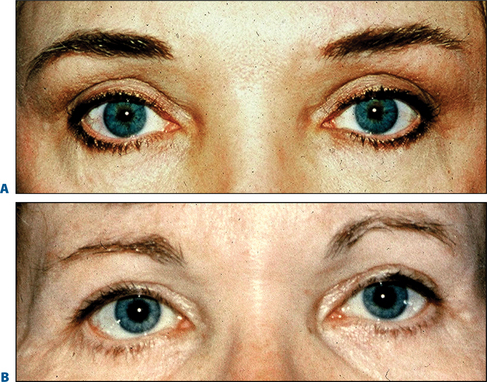
The importance of the lower eyelid-cheek junction has been appreciated by plastic surgeons over the past decade. In the early 1970s and 1980s, the standard surgical treatment for ‘tired eyes’ consisted of removal of fat and skin or skin and muscle from the lower eyelids.6 This universally produced either an unattractive vertical shortening of the lower lid or an accentuated hollowness under the eyes or both (Fig. 20-5). By the 1990s patients and surgeons alike began to realize that this original technique contributed to a haggard, unattractive periorbital appearance of aging.
Suborbital maxillary volume/malar suborbital deficiences
A medial sulcus just lateral to the nasal pyramid, which extends distally for 2.5 cm obliquely towards the angle of the mandible, has been termed a ‘nasojugal’ sulcus or ‘tear trough.’7,8 However, either by heredity or mainly with aging changes, this suborbital depression continues beneath the entire lower eyelid. This volume deficiency is not at the level of the inferior orbital rim as originally thought by plastic surgeons. Instead, it occurs consistently at a measured distance of 8 to 10 mm below the orbital rim. This observation was made by me early in the 1980s, when postoperative blepharoplasty patients began complaining about their more tired, ‘hollow’ look.
The etiology of why such a depression in this area appears as early as the third decade of life and certainly by the late 40s and early 50s has been unclear. Recently, however, largely through the photographic and computer studies of Lambros,4 it is now agreed upon that a true atrophy or involution of fat occurs in the upper two-thirds of the face and largely in the periorbital region. This disappearance of fat correlates with the increased appearance of a suborbital hollowness, which creates a tired, haggard appearance.
The treatment of the suborbital sulcus has been evolving for at least 25 years. In 1983, prompted by complaints of patients about the increased hollowness of their orbital region from traditional blepharoplasty I began transplanting autogenous tissues such as fat, temporalis fascia, temporalis muscle, and galea into the suborbital region below the orbital rim behind the orbicularis oculi muscle and over the SOOF tissues9 (Fig. 20-6). This area has now become recognized as the true area of deficiency, which produces a tired appearance from the fat atrophy, which accompanies aging.
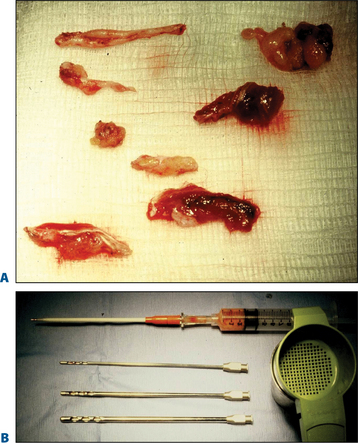
Figure 20-6 A, Pieces of temporalis fascia, temporalis muscle and galea. B, Aspirated autologous fat.
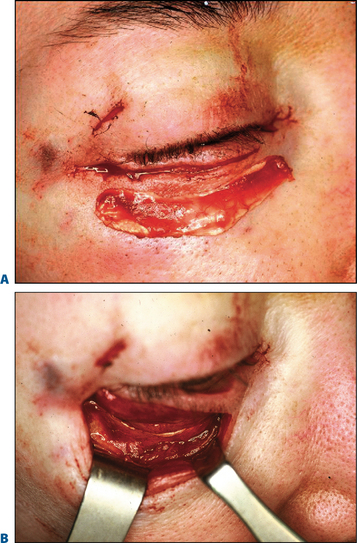
My tissue transfer technique when a lower blepharoplasty was performed for ‘fat bags,’ the fat was excised tangentially from lateral to medial canthus, leaving a medial vascular pedicle. A small instrument such as a curved hemostat was introduced beneath the orbicularis muscle to tunnel from lateral to medial, grasping the fat pedicle and pulling it into the suborbital sulcus. When upper eyelid surgery was performed simultaneously, the strip of orbicularis muscle routinely removed, was also placed into the suborbital sulcus in a similar fashion. When combined with rhytidectomy, the author often used segments of temporalis fascia including muscle or even large amounts of galea and on occasion ear cartilage (Fig. 20-7). These procedures were performed in 150 to 200 patients at that time.
Although these transplantation methods could be demonstrated in the long-term (see photographs at six months to one year, Figs 20-8 & 20-9) the results were only partially successful in improving the suborbital sulcus with volume addition, assessed at a 50–70 percent improvement, 50–70 percent of the time. Lumps and irregularities using these tissue transplantation techniques were infrequent because the tissues were carefully distributed beneath the thickness and padding of the intact orbicularis muscle.


In 1998 Hamra10 (evolving from the work of Loeb),11 developed zygo-orbicular complex dissection techniques. At the same time subperiosteal midface suspension procedures evolved.2 These newer dissections elevated the orbicularis in the cheek above or below the periosteum and fat could be transposed over the orbital rim and sutured into the SOOF.12 A further refinement was the release and reset of the orbital septum.13
Elimination of the ‘tired look’ is very adequately accomplished with upper midface suspension because it provides the advantage of elevating the lower, thicker tissues of the cheek up over the thin suborbital sulcus adding additional thickness to the transposed fat thus providing a most consistent and excellent blending of the lid-cheek junction (Figs 20-10 & 20-11). A suborbital tear trough malar implant with transverse dimensions of 6 cm, a vertical dimension of 3.2 cm and a thickness of 3 or 4 mm will also blend the lid–cheek junction well without the need for an extensive midface submalar and lateral orbital temple brow dissection required for an upper and mid face ‘lifting’ procedure.


The alloplastic solution
In the early 1980s, I conceived of an implant designed to fill the inferior orbital rim and suborbital sulcus. Flowers by the 1990s8 carried this thought forward and his present day tear trough implants were developed and are obtainable through Implantech Corporation, Ventura, California.
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


