Aging Upper Face (Brow and Lids)

Description
Glabellar frown lines and periorbital rhytids
Asymmetric brow position.
Excess upper lid skin.
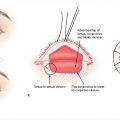
Tear trough deformity
Midface decent with prominent nasolabial folds
Work-up
History
Identify medical conditions that may increase the risk for complications.
Blepharochalasis, Graves disease, benign essential blepharospasm.
Rosacea, pemphigus, sarcoidosis.
Previous periorbital and facial procedures.
Assess for a history of dry eyes.
Blepharoplasty may worsen a previous history of dry eyes.
Contact lenses: If patient is able to use contact lenses comfortably, there is no history of dry eyes and tear production is normal.
Recent LASIK surgery: Should not undergo blepharoplasty for at least 6 months following procedure.
Postmenopausal hormone replacement therapy (HRT)
70% higher risk for dry eye.
Additional 15% increase in risk for dry eye every 3 years during HRT.
Physical examination
Forehead analysis
Position of anterior hairline
Shape and slope of forehead
Transverse forehead and glabellar rhytids
Brow analysis
Eyebrow shape: Should be a gentle curve with the medial and central portions wider than the lateral aspects.
Eyebrow peak: Should be located at or just lateral to the lateral limbus.
Eyebrow location: Brow peak should be 1 cm above supraorbital rim in women and at supraorbital rim in men.
Brow ptosis:
may be compensated by hyperactivity of frontalis muscle. Immobilize frontalis and ask patient to open eye and assess brow position.
Lateral extension of upper lid hooding onto periorbital region is a marker of forehead ptosis (Connell sign).
Eyelid analysis
Upper lid:
Excess skin, fat herniation, lacrimal gland prolapse
Lid position: should not be lower than 2 mm from superior limbus.
Supratarsal fold position: measure margin-crease distance. Normal 7 to 11 mm. High position indicates levator dehiscence.
Levator function: measure eyelid excursion from maximal down gaze to extreme up gaze while stabilizing the brow.
Cover test: to unmask sub-clinical ptosis if there is asymmetric lid position.
Lower lid
Excess skin, fat herniation, tear trough
Lid position: lower lid should not be below inferior limbus
Lid laxity: lid distraction more than 6 mm requires canthal procedures.
Snap back test: after distraction lower lid should immediately snap back to its position
Position of eye in relation to orbital rim: positive vs negative vector.
Lateral canthal position:
Lateral canthus is positioned slightly superior to medial canthus (positive canthal tilt) by an average of 4 degrees.
Negative canthal tilt may require canthopexy.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


