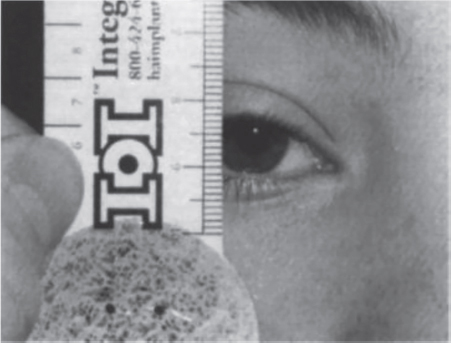
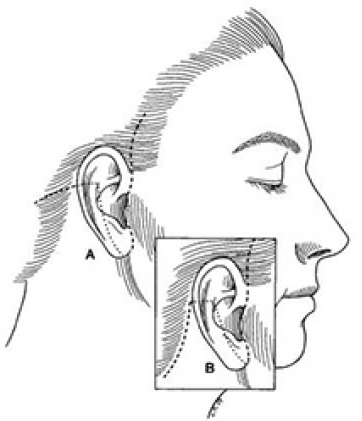
10 Aesthetic Surgery for the Aging Face Abstract This chapter will review analysis of and surgical options for the aging face, including blepharoplasty, brow lift, and facelift. The reader will be able to analyze the aging face and propose appropriate surgical intervention, and manage postoperative events such as skin flap loss and retrobulbar hematoma. Keywords: aesthetic surgery, aging face, facelift, facial rejuvenation Six Key Points • Facial analysis should proceed from cranial to caudal in thirds • Pay close attention to the eyes in the aging face. • Rejuvenation must address volume loss • Neuropraxias are observed, but visualized nerve injuries are repaired. • Skin slough is managed conservatively. • Initial masnagement of any outcome that can be attributed to scarring is scar massage and observation. A 64-year-old woman presents for rejuvenation of the face. 1. What do you see? The face is evaluated for overall skin quality, sun damage, and presence of rhytids. It is then evaluated from cranial to caudal. The forehead is evaluated for rhytids as well as relative length and location of the hairline, which can have implications for forehead shortening and incision placement for a brow lift. The brow is noted for its position, and any brow ptosis is noted. The eyes are evaluated for dermatochalasis and ptosis, as well as any indicators of eyelid disease or general health from the sclera, such as diffusely injected sclera, or scleral icterus. The position and tone of the lower lids is noted, as well as the vector of the eye. The nasolabial folds are noted, and their relative prominence, as are perioral rhytids and the presence of marionette lines. Overall atrophy of facial soft tissue is noted. 2. What do you offer the patient? A facelift is the most appropriate intervention to address mid- and lower face descent. I would offer a superficial musculoaponeurotic system (SMAS) plication facelift. If the patient also has brow and eyelid issues, it is offered as a staged approach—first the brow and the eyelids, then the face and neck, and finally laser resurfacing if indicated. 3. Explain why an SMAS plication is offered and draw your incision. See Fig. 10.1 for incisions. The incision goes from the temporal hairline to a pretragal incision, wrapping around the earlobe to extend posteriorly into the hairline. There are several techniques for a facelift, including a skin-only facelift, in which the SMAS layer is not addressed, an SMAS-ectomy, in which redundant muscle is removed, and other variations. A skin-only facelift will not address the muscle and the differential vectors of descent. Because of the path of the facial nerve branches, which lie on the sub-SMAS level, resecting SMAS not only uses the volume of the SMAS layer, but also runs the risk of injuring the facial nerve branches. An SMAS plication will preserve volume while avoiding facial nerve branches. The SMAS plication is performed over the zygoma, and the zygomatic retaining ligaments and mandibular retaining ligaments must be released to reposition the skin over the plicated SMAS. Fig. 10.1 Incision placement for a facelift. SMAS, superficial musculoaponeurotic system. From Wobig JL, Dailey RA. Oculofacial Plastic Surgery: Face, Lacrimal System, and Orbit. New York, NY: Thieme Medical Publishers; 2004. 4. What do you do about the neck? A separate, approximately 4 cm, submental incision is used. This incision is placed posterior to the submental crease, between the mentum and hyoid, because placement within the submental crease can create a persistent double chin deformity. This separate incision allows for access to the anterior neck. If there is platysmal banding, the dissection proceeds in the intermediate plane of the neck. Facelift scissors are used to create skin flaps. Excess fat can be directly excised, as long as at least 5 mm of fat is left on the skin. The platysma muscle is exposed to the boundaries of thyroid cartilage subplatysmal fat, anterior bellies of the digastric muscles, and submandibular glands. In this dissection, there is release of the submental retaining ligaments. The anterior bellies of the digastric muscles can be excised if needed, or they can be plicated, followed by platysmal plication.1 The space is irrigated, and the submental incision is closed last, after hemostasis has been obtained under the facelift flaps. 5. Postoperatively, she calls to report that she has swelling on the left side of her face. What do you do? The first step is to bring her in to evaluate her and exclude a hematoma, which can occur approximately 4% of the time. Even if there are drains in place and a compression dressing, a hematoma can occur. Because a hematoma can affect the viability of the skin flaps, it is important to identify it and drain it. If she has a hematoma on examination, plan operative intervention by obtaining informed consent and alerting the operating room staff. The hematoma is evacuated surgically and potential causes of bleeding are identified. Once hemostasis has been confirmed, the incisions are reclosed. 6. What other things would you do? Risk factors for hematoma are high blood pressure, medications or herbal supplements that decrease clotting ability, and traumatic events such as shear injury, which may disrupt a clot. Thus, I would ensure that she is normotensive, that, she is not taking any medication that may decrease clotting ability, and that drains and compression dressing are replaced. If the hematoma is a late presentation, and there is suspicion that it has liquefied, which can happen in about a week, the hematoma can be aspirated in the office. 7. She complains of decreased movement of her lower lip. What do you do? Facial nerve injuries can happen in a face lift and are part of the informed consent process. Initially, I would wait because it may represent a neuropraxia, and I would counsel her that it may recover on its own. Use of a sub-SMAS dissection plane increases the risk of a nerve injury four-fold. If a nerve injury is identified intraoperatively, it should be repaired in the operating room. 8. How do you repair the nerve? The repair is done with microsurgical instruments, and with microscopic magnification. The two ends of the nerve are identified. The branch can be confirmed with a nerve stimulator, which will work up to approximately 72 hours after surgery, and an epineural repair is performed with 8–0 or 9–0 nylon. 9. She comes back a week later and she has skin slough. What do you do? It is managed conservatively with ointment such as Bacitracin. Silver sulfadiazine is avoided because it can cause skin darkening. The area is allowed to heal by secondary intention. 10. It is possible to excise that area and do a small rotational flap, which she hopes will get her healed sooner. Despite pressure from the patient, it is still appropriate to manage it conservatively. A 67-year-old woman presents for eyelid rejuvenation. 1. What do you see? The eyes are assessed beginning at the brows. It is important to note whether the brow is in good position, which is at the supraorbital rim in men and slightly above it in women, and to note whether it is in place because of compensatory frontalis contraction, which may indicate underlying brow ptosis. Eyelids should be assessed for excess skin as well as blepharoptosis, which is measured by the marginal reflex distance (Fig. 10.2). The elasticity of the lower lid should be measured by the snap-back test and the pinch test (Table 10.1). In addition, Bell’s phenomenon should be assessed. A history should include assessment for dry eyes and the use of eye drops, and physical examination may include Schirmer’s test (Table 10.2). 2. How is Schirmer’s test performed? As in Table 10.1, a paper strip is placed in the inferior fornix for 5 minutes. The distance that a tear film has traveled is measured on the strip. Normal is greater than 15 mm. Postoperatively, tear flow can be disrupted, and dry eyes can be exacerbated. 3. What do you offer the patient? In a patient with brow ptosis, dermatochalasis, and lower lid laxity and redundancy, a brow lift and upper and lower blepharoplasty are offered. An endoscopic brow lift is offered for patients without significant forehead elongation and with mild forehead rhytids. The procedure is done under monitored anesthesia care or under general anesthesia. The port sites are marked in horizontal positions at the midline, 0.5 cm posterior to the hairline, and laterally in the temple area 7 and 10 cm from the midline and approximately 2 cm posterior to the hairline. The forehead is injected with local anesthetic with epinephrine 1:100,000 and the incision site in the hair-bearing regions are injected with local anesthetic with epinephrine 1:200,000. The lateral-most port site is incised with a knife, and the most lateral incision is continued to the deep temporal fascia, which is then further exposed with a baby Metzenbaum scissors. The access port is placed to expose the plane between the superficial and deep temporal fascia. A periosteal elevator is used to sweep toward the more medial incision, which is medial to deep temporal fascia and at the level of periosteum, which is incised such that the plane of dissection is subperiosteal. The midline incision is made after the lateral incisions are made and the sites connected. A 30-degree 4-mm endoscope is placed in the lateral-most incision. A periosteal elevator is used to dissect in the subperiosteal plane to the supraorbital rim, and proceeds from lateral to medial. The supraorbital and supratrochlear nerves are identified, and a grasper is used to remove the corrugator muscle. The procedure is repeated on the opposite side, and fat grafts are taken from a rent in the deep temporal fascia cephalad to the medial aspect of the zygomatic arch. Hemostasis is obtained. A fascial suspension suture is placed through the superficial temporal fascia of the lateral-most incision, and secured to the posterior aspect of the incision. If needed, a second suspension suture is placed through the more medial incision, and passed through a bone tunnel made by a 1.1-mm burr with entrances 4 mm apart and 4 mm deep. Endotine can also be used at this point for additional fixation. A small drain is placed, and the incisions are closed in layers.
Questions
Case 1
Case 2
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine