Introduction
Aesthetic medicine comprises all medical procedures that are aimed at improving the physical appearance and satisfaction of the patient, using noninvasive to minimally invasive cosmetic procedures.
These aesthetic procedures consist of:
- ▪
injections of neurotoxins
- ▪
dermal fillers/fat grafting
- ▪
chemical peels
- ▪
radiofrequency
- ▪
cryotherapy
- ▪
lasers and intense pulsed light (IPL)
- ▪
ultrasound treatment
- ▪
platelet-rich plasma (PRP)
The author used a combination of these procedures for nonsurgical rejuvenation. This chapter provides an overview of each of these with their clinical implications, recommended indications, management, advantages, and disadvantages.
Multimodality Nonsurgical Rejuvenation With a Regional Approach
Botulinum Toxin (Botox)
In aesthetic medicine botulinum toxin (see Table 2.1 and Fig. 2.1 ) is the most commonly used nonsurgical treatment worldwide. In 2014, 4.89 million Botox treatments were done worldwide. Its popularity is due to its excellent safety record and predictable outcomes.
| Dynamic rhytids |
|
| Diminishing the depressor activity of certain muscles |
|
| Hypertrophic muscles |
|

Commercially available botulinum toxin A are:
- ▪
onabotulinum toxin A (Botox)
- ▪
abobotulinum toxin A (Dysport)
- ▪
incobotulinum toxin A (Xeomin)
Dilution
- ▪
1 B.U. = 2.5 s.U
1 vial of Dysport (500 s.U) + 2.5 mL saline = 20 U/0.1 mL
(can be rediluted in the syringe with 1 : 1 ratio to create a concentration of 10 s.U/0.1 mL)
- ▪
1 vial of Botox (100 U) + 2.5 mL of saline = 4 U/0.1 mL
30- to 32-gauge needle (a smaller needle is preferred in sensitive patients)
4 U Botox = 10 U Dysport
Preprocedure Management of Neuromodulators
- ▪
Conduct an assessment of the patient.
- ▪
Note the location and depth of rhytids.
- ▪
Obtain a history of the patient’s concerns.
- •
Brow position is important.
- •
Check for the presence or absence of compensatory brow elevation.
- •
Check for blepharochalasis and dermatochalasis.
- •
Check for collagen depletion.
- •
Measure the width of the forehead (a wide forehead would need more neuromodulator/Botox).
- •
Assess strength of frontalis muscle and length of corrugator.
- •
- ▪
Take a preoperative photograph.
- ▪
Apply a eutectic mixture of local anesthetics (EMLA) 30 minutes prior to procedure.
- ▪
Give counseling about potential complications.
- ▪
Obtain consent.
Postoperative Care for Neuromodulators
- ▪
The lumps on the area injected will go down in 15 to 30 minutes.
- ▪
Do not rub or apply pressure on the area that was injected with Botox.
- ▪
For 6 hours, avoid bending or stooping down; instead lie down flat on your back.
- ▪
Do not go to the gym or do any sports until the next day.
- ▪
Follow up after 10 days.
- ▪
Take a postoperative photograph.
Hyaluronic Acid (Fillers)
Adding volume along with short-scar face lift has largely overtaken surgical correction for midface. The choice of filler is dependent on the anatomy of each individual and the specific treatment goals. Injectable soft-tissue fillers are durable, well tolerated, and potentially reversible in unfavorable clinical outcomes. Small-particle hyaluronic acid (HA) with lidocaine (Restylane Silk, Galderma, Uppsala, Sweden) is used for submucosal implantation for lip augmentation and dermal implantation for correction of perioral rhytids. Side effects are generally mild and transient.
Preprocedure Management
- ▪
Conduct a general assessment of the patient.
- ▪
The patient should avoid aspirin (any product containing acetylsalicylic acid), vitamin E, and other dietary supplements, including gingko, evening primrose oil, garlic, feverfew, and ginseng, for 2 weeks.
- ▪
The patient should also avoid blood thinners such as aspirin, ibuprofen (Advil, Motrin), and naproxen (Aleve, Naprosyn) 1 week before the treatment.
- ▪
Enquire about history of cold sores (or fever blisters) prior to treatment.
- ▪
Optionally, the patient can start taking an Arnica tablet for 1 week prior to treatment and 4 days posttreatment. The standard dosage is three Arnica tablets (30 CH) three times a day 30 minutes before or after a meal.
- ▪
Enquire about allergy or sensitivity to lidocaine.
- ▪
Mild bruising is common and can last 7 to 14 days.
- ▪
Take a preoperative photograph.
- ▪
Apply EMLA 30 minutes prior to the procedure.
- ▪
Give counseling about potential complications and obtain consent.
Postoperative Management
- ▪
Follow up after 2 weeks for touch-up.
- ▪
Take a postoperative photograph.
- ▪
Counsel the patient that the volume will go down by approximately 20%.
- ▪
Give Voltarol for pain relief.
- ▪
Massage with Arnica.
- ▪
Avoid hot beverages after the dental block (for lip augmentation).
- ▪
Avoid cold compression to prevent headache (in the temporal area).
- ▪
Minimize movement of the treated area.
- ▪
Avoid applying heat to the treated area until bruising or any swelling has resolved.
- ▪
On the day of treatment, avoid activities that cause facial flushing including consuming alcohol, hot tub or sauna use, exercising, hot wax, and tanning. Avoid extreme-cold activities, like skiing or hiking outdoors.
- ▪
Gently apply a cool compress or wrapped ice pack to the treated areas for 15 minutes every few hours as needed to reduce discomfort, swelling, or bruising up to a few days after treatment. When bruising occurs it typically resolves within 7 to 14 days.
- ▪
Results last approximately 6 to 12 months.
- ▪
For more than 4 cc of filler used, prednisolone 40 mg with Nexium 40 mg daily for 2 days after meals may be considered.
Upper Face
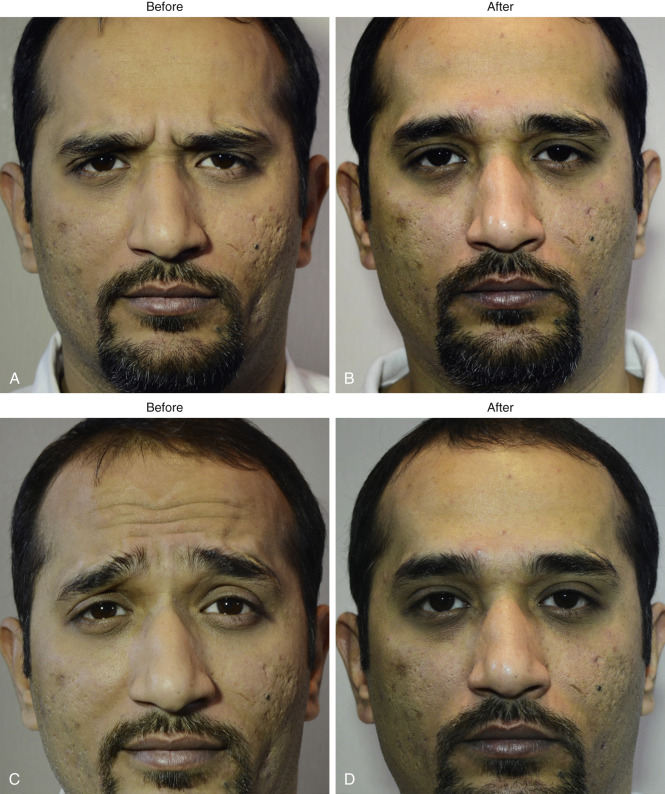
Forehead and Brow Rejuvenation ( Fig. 2.2 )
Assessment ( Table 2.2 )
- ▪
Check the brow position (this is important).
- ▪
Check for the presence or absence of compensatory brow elevation.
- ▪
Check for blepharochalasis or dermatochalasis.
- ▪
Check for collagen depletion.
- ▪
Assess the strength of muscle.
- ▪
Measure the width of the forehead.
| Indication/patient’s perspective | Muscle | Plane | Treatment |
|---|---|---|---|
| Glabellar frown lines | Corrugator | Subdermal | 4–8 injections in females 6-10 injections in males 10 s.U in each injection |
| Glabellar frown lines | Procerus | Deep subdermal | |
| Glabellar frown lines | Depressor supercilli | Deep subdermal | |
| Dynamic lines on the forehead | Frontalis | Subdermal | One injection centrally and two laterally on forehead. (between 10 and 30 s.U in divided doses) |
| To maintain the brow position To prevent lateral brow ptosis | Orbicularis oculi (superior lateral fibers) | Subdermal | As a prophylactic measure, 10 s.U on each side to be given under the tail of the brow to inactivate the depressor action |
Technique
- ▪
The brow elevator (frontalis) and depressors (corrugator, procerus, depressor supercilli [DSC] for the medial brow and the superolateral fibers of the orbicularis oculi for the lateral brow) should be treated as a single unit to prevent brow ptosis.
- ▪
Preventing brow ptosis should be the priority.
- ▪
This can be achieved by full treatment to the corrugator, procerus, and DSC, a conservative dose to the frontalis, and a later touch-up to the frontalis if required in 10 days.
- ▪
Treatment of the superolateral fibers of the orbicularis oculi will also help to maintain an elevated brow position.
- ▪
Assess the activity of DSC. If DSC overactivity is missed, the patient may come back with descent of the medial brow (an angry look).
- ▪
If there is previous history of heaviness of brow after treatment, inject only in the central forehead.
- ▪
For the technique, see .
- ▪
Injections placed above the midpupillary line for the corrugator should be at least 1 cm above the bony orbital rim to help prevent lid ptosis caused by diffusion of Botox to levator muscles.
- ▪
Some return for a touch-up in 10 days.
Complications
- ▪
Lid ptosis
- ▪
Brow ptosis
Periocular Rejuvenation (see Table 2.3 , Fig. 2.3 , and )
| Patient characteristics | Management |
|---|---|
| Dark circles |
|
| Prominent eye bags |
|
| Prominent eyes |
|
| Sleep lines |
|
| Upper lid hollowness and brow position |
|
| Periocular rhytids |
|
| Muscle | Plane | Treatment |
|---|---|---|
| Orbicularis oculi | Subdermal | 1 cm lateral to the lateral orbital rim 4–6 injections each side 10 s.U in each injection |
| Pretarsal orbicularis (bulge under the eyes during smile) | Subdermal | Infraorbital injection 5–10 s.U under the eyes into the pretarsal fibers on each side in divided doses |
| Bunny lines | Subcutaneous | One injection (5–10 s.U) high on each side of the nasal sidewall (form a bleb) |

Upper Face
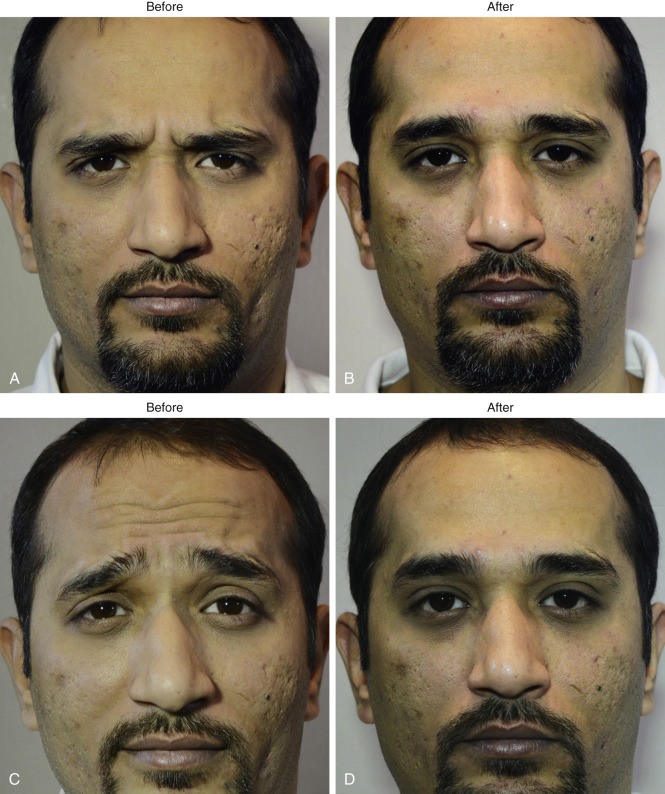
Forehead and Brow Rejuvenation ( Fig. 2.2 )
Assessment ( Table 2.2 )
- ▪
Check the brow position (this is important).
- ▪
Check for the presence or absence of compensatory brow elevation.
- ▪
Check for blepharochalasis or dermatochalasis.
- ▪
Check for collagen depletion.
- ▪
Assess the strength of muscle.
- ▪
Measure the width of the forehead.
| Indication/patient’s perspective | Muscle | Plane | Treatment |
|---|---|---|---|
| Glabellar frown lines | Corrugator | Subdermal | 4–8 injections in females 6-10 injections in males 10 s.U in each injection |
| Glabellar frown lines | Procerus | Deep subdermal | |
| Glabellar frown lines | Depressor supercilli | Deep subdermal | |
| Dynamic lines on the forehead | Frontalis | Subdermal | One injection centrally and two laterally on forehead. (between 10 and 30 s.U in divided doses) |
| To maintain the brow position To prevent lateral brow ptosis | Orbicularis oculi (superior lateral fibers) | Subdermal | As a prophylactic measure, 10 s.U on each side to be given under the tail of the brow to inactivate the depressor action |
Technique
- ▪
The brow elevator (frontalis) and depressors (corrugator, procerus, depressor supercilli [DSC] for the medial brow and the superolateral fibers of the orbicularis oculi for the lateral brow) should be treated as a single unit to prevent brow ptosis.
- ▪
Preventing brow ptosis should be the priority.
- ▪
This can be achieved by full treatment to the corrugator, procerus, and DSC, a conservative dose to the frontalis, and a later touch-up to the frontalis if required in 10 days.
- ▪
Treatment of the superolateral fibers of the orbicularis oculi will also help to maintain an elevated brow position.
- ▪
Assess the activity of DSC. If DSC overactivity is missed, the patient may come back with descent of the medial brow (an angry look).
- ▪
If there is previous history of heaviness of brow after treatment, inject only in the central forehead.
- ▪
For the technique, see .
- ▪
Injections placed above the midpupillary line for the corrugator should be at least 1 cm above the bony orbital rim to help prevent lid ptosis caused by diffusion of Botox to levator muscles.
- ▪
Some return for a touch-up in 10 days.
Complications
- ▪
Lid ptosis
- ▪
Brow ptosis
Periocular Rejuvenation (see Table 2.3 , Fig. 2.3 , and )
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


