This article will offer an in-depth review of the current literature focusing on male esthetic genital surgery. After a thorough discussion of the anatomy, we will focus on the literature involving the advancement of nonsurgical male genital enhancement procedures, which includes the individual enhancement of the glans penis, scrotum, and penile shaft, in addition to the treatment of complications that may develop from these procedures. This is followed by a review of the literature surrounding surgical male genital enhancement procedures that include the use of autologous tissue and implants. Following this, we discuss specific male genitalia abnormalities.
Key points
- •
Anatomy of the penis is imperative to understand for the proper management of functional and aesthetic issues regarding the penis.
- •
Nonsurgical procedures involving injectable materials such as liquid silicone, hyaluronic acid, and polymethyl-methacrylate microspheres have shown some effectiveness in girth enhancement, yet they pose significant risks such as foreign body reactions and complications such as arterial embolization.
- •
Dermal-fat grafts are often used to address both girth and length enhancement. The grafts are designed to provide structural support and volume, achieving a more natural appearance.
- •
Penoscrotal webbing, characterized by excessive skin between the penis and scrotum causing cosmetic, discomfort, and functional issues, is classified based on its extent and thickness, offering surgical options such as V-Y or Z-plasty techniques tailored to individual severity and patient needs, aiming to improve both appearance and function while minimizing complications.
- •
The diagnosis of micropenis, defined by a penile length less than −2.5 standard deviations from the average, can result from various factors, including structural or hormonal issues, congenital syndromes, or acquired conditions such as buried penis due to obesity or medical ailments, leading to tailored surgical treatments for aesthetic or functional concerns, including penile lengthening and phalloplasty procedures using different flap techniques for reconstruction and restoration of sensation and function.
Introduction
Self-perception as it relates to the appearance of genitalia plays a significant role in a male’s sexual identity and greatly influences his self-esteem. This perception is often influenced by outside factors such as social media, pornographic material, and existing relationships, which oftentimes can cause a skewed misconception of what is considered “normal” male genitalia. This misconception often includes the belief that “thicker and longer” male genitalia is preferred and the gold standard. As such, many men present for both surgical and nonsurgical aesthetic genital procedures in an effort to alter not only the aesthetic appearance of their genitalia but also the sexual function. This article will offer an in-depth review of the current literature focusing on male aesthetic genital surgery. After a thorough discussion of the anatomy, we will focus on the literature involving the advancement of nonsurgical male genital enhancement procedures, which includes the individual enhancement of the glans penis, scrotum, and penile shaft, in addition to the treatment of complications that may develop from these procedures. This is followed by a review of the literature surrounding surgical male genital enhancement procedures, which include the use of autologous tissue and implants including complications resulting from these procedures and their treatment. In addition, we will discuss specific male genitalia abnormalities: penoscrotal web, micropenis, and buried penis with a detailed discussion of surgical treatment options for these abnormalities.
Significance/in-depth analysis of topic
Male Genital Anatomy
Surface anatomy
The penis is subdivided into 3 main segments: the base, the body, and the glans. The base of the penis is the most proximal and fixed portion of the penis. Although this portion of the penis is in the superficial perineal pouch of the pelvic floor and is not visible externally, it serves as the base of the entire structure. The body, or shaft, of the penis is suspended from the pubic symphysis and is located between the root and the glans. The glans is cone-shaped, and the most distal part of the penis that is formed by the distal expansion of the corpus spongiosum. The proximal portion of the glans is known as the corona, whose neck separates the structure from the body of the penis. Most distally on the glans penis is the urethral meatus [ ].
The skin of the shaft of the penis is thin, pliable, and more heavily pigmented than that of the rest of the body, allowing for erection. It is continuous with the prepuce, which connects to the underlying fascia by loose connective tissue and to the surface of the glans by the frenulum, a median fold on the ventral surface of the penis [ , ]. The prepuce is a dual layer of retractable tissue that is typically removed during circumcision.
The scrotum contains the external spermatic fascia, testes, epididymis, and spermatic cord. It is divided into 2 compartments by a scrotal septum and consists of a parietal layer that lines the smooth muscle of the sac and visceral layer that lines the testis and epididymis [ ].
Musculature
A total of 4 muscles are located in the penis. These muscles comprise of the paired bulbospongiosus, which are associated with the bulb of the penis, and the paired ischiocavernosus, which are located in the base of the penis. The bulbospongiosus cross the pelvic outlet and support the perineal body and pelvic viscera. Its contraction empties any residual semen and urine out of the spongy urethra. Anterior muscle fibers of this muscle aid in maintaining an erection by increasing the pressure inside the bulb of the penis. The ischiocavernosus muscles surround the right and left crura and help maintain an erection by contracting to force blood from the cavernous spaces of the crura into the distal parts of the corpora cavernosa. Both muscle pairs compress the deep dorsal veins, preventing drainage of the cavernous spaces and thus maintaining an erection [ , ].
The scrotum is a fibromuscular structure that contains the dartos and cremasteric muscles. The dartos muscle is a smooth, thin sheet of muscle that is located just underneath the skin of the scrotum. The cremasteric muscle is a paired muscle, with medial fibers originating from the pubic tubercle and lateral fibers originating from the internal oblique. This muscle serves mainly a protective function to the testes and other structures located within the sac [ ].
Erectile tissues
The base and body of the penis are spanned by 3 masses of erectile tissue that fill with blood during sexual arousal to produce an erection. In the base of the penis, these erectile tissues are the right and left crura and the bulb, with the bulb lying in between the 2 crura. As these structures continue into the body of the penis, the 2 crura join dorsally to form the corpora cavernosa ( Fig. 1 ). Ventrally, the bulb becomes the corpus spongiosum, eventually expanding to become the glans penis. The bulb, corpus spongiosum, and glans contain the male urethra throughout. In order to prevent the urethra from occlusion during an erection, the corpus spongiosum fills to a reduced pressure as compared with the cavernosa [ ].
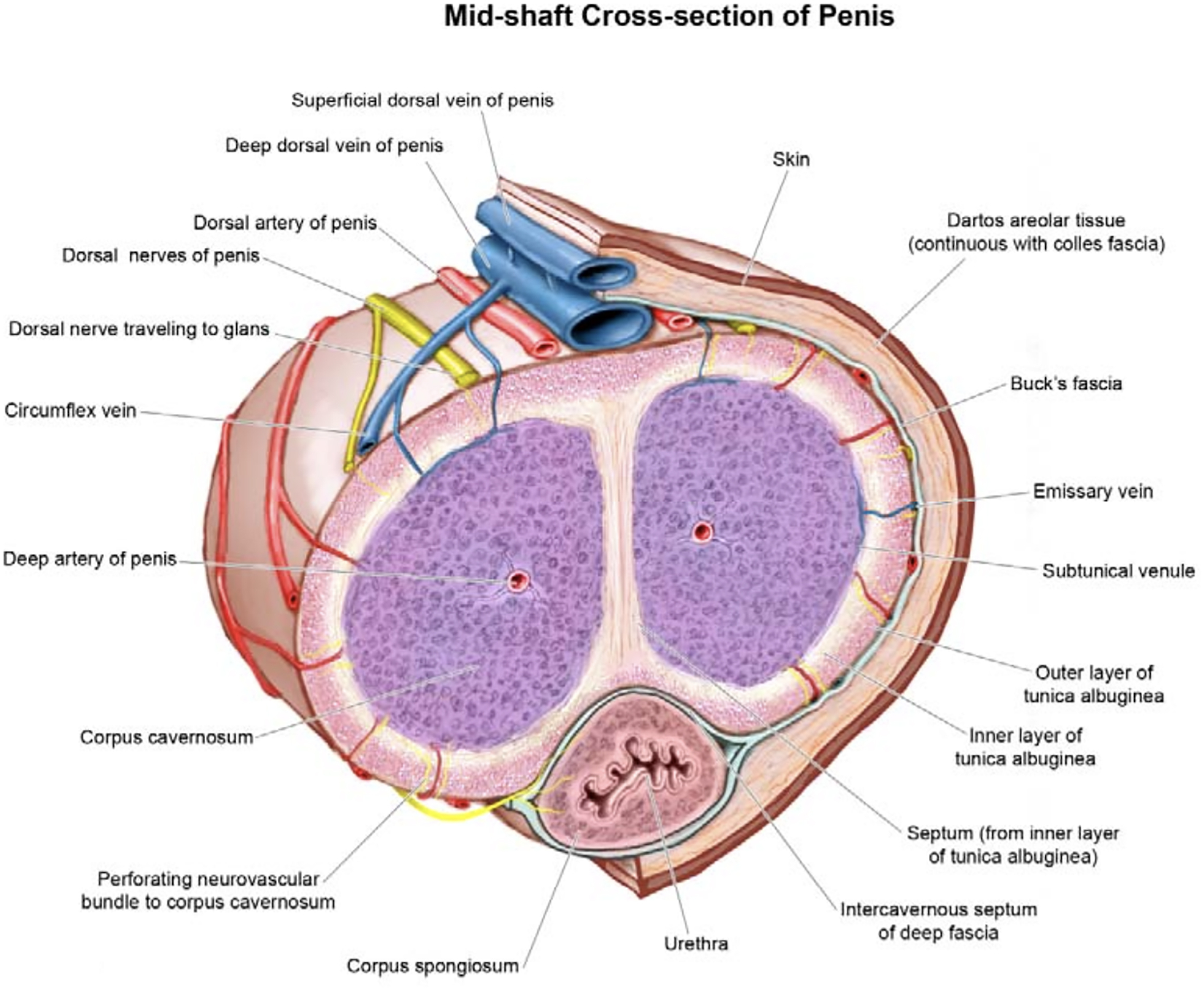
Fascial coverings
Each mass of erectile tissue is surrounded by layers of fascia. The tunica albuginea is a sturdy layer of fascia that surrounds each cavernous body. The next layer of fascia is called Buck fascia, otherwise known as the deep fascia of the penis. Buck fascia is a continuation of the deep perineal fascia and surrounds all 3 erectile bodies, holding them together. Immediately under the skin and the most superficial layer of fascia is called Colles fascia, which is a continuation of Scarpa fascia that covers the abdominal wall [ ].
Ligaments
At the root of the penis, 2 ligaments act to anchor the penis to the pubic symphysis. The suspensory ligament is a condensation of Buck’s deep fascia that connects the erectile bodies of the penis and the fundiform ligament is a condensation of abdominal subcutaneous tissue that runs along the linea alba that surrounds the penis like a sling. Both structures provide additional support to the penis. These are the ligaments transected at the time of a penile lengthening procedure [ ].
Vascular anatomy of male genitalia
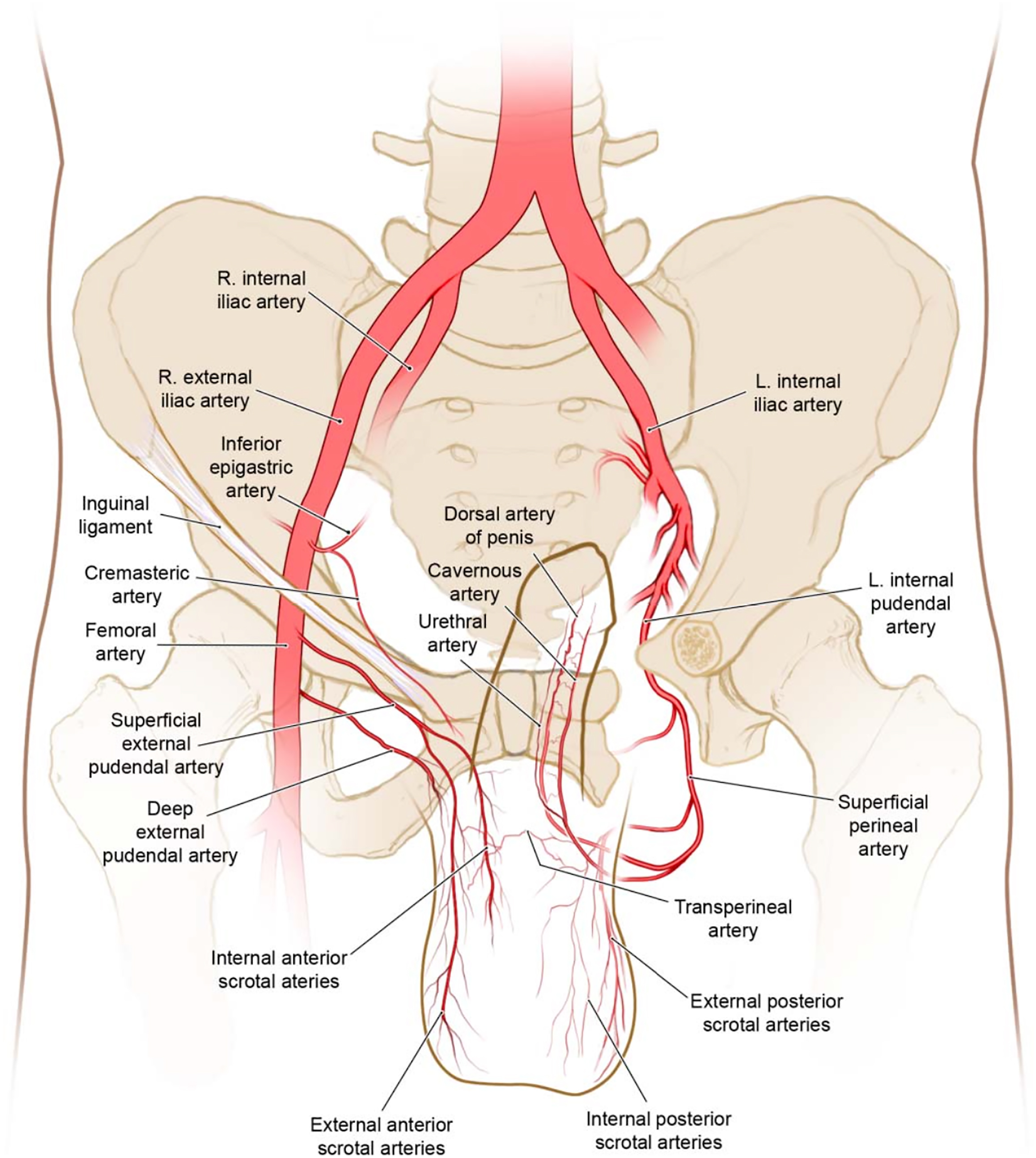
The male genitalia is supplied almost entirely by branches off of the internal and external pudendal arteries, which originate from the anterior division of the internal iliac artery ( Fig. 2 ).
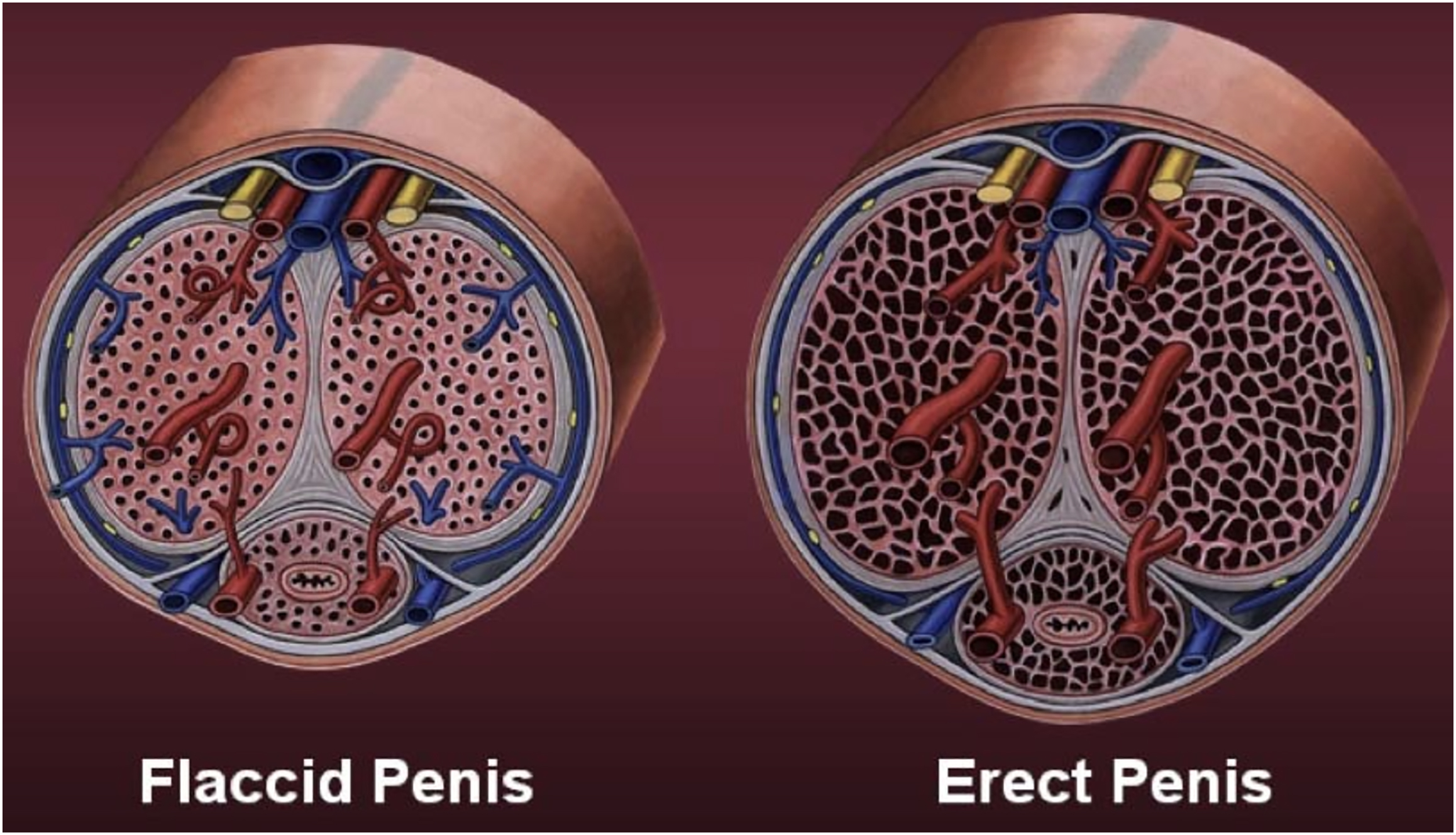
The arterial supply of most of the penis is through the dorsal arteries of the penis, the deep arteries of the penis, the helicine arteries, and the bulbourethral artery, all of which branch off of the internal pudendal artery ( Fig. 3 ) [ , ]. Only the penile skin is supplied by branches of the external pudendal arteries [ ]. The dorsal artery of the penis runs between the corpora cavernosa to supply the fibrous tissue of the erectile bodies and the penile skin, whereas the deep arteries of the penis run within the body of each corpora cavernosa to supply the erectile tissue. The helicine arteries of the penis are branches that come off the deep arteries of the penis. They are taught during an erection and coiled when the penis is flaccid ( Fig. 4 ) [ ]. The bulbous part of the corpus spongiosum, urethra, and bulbourethral gland are supplied by the bulbourethral artery.
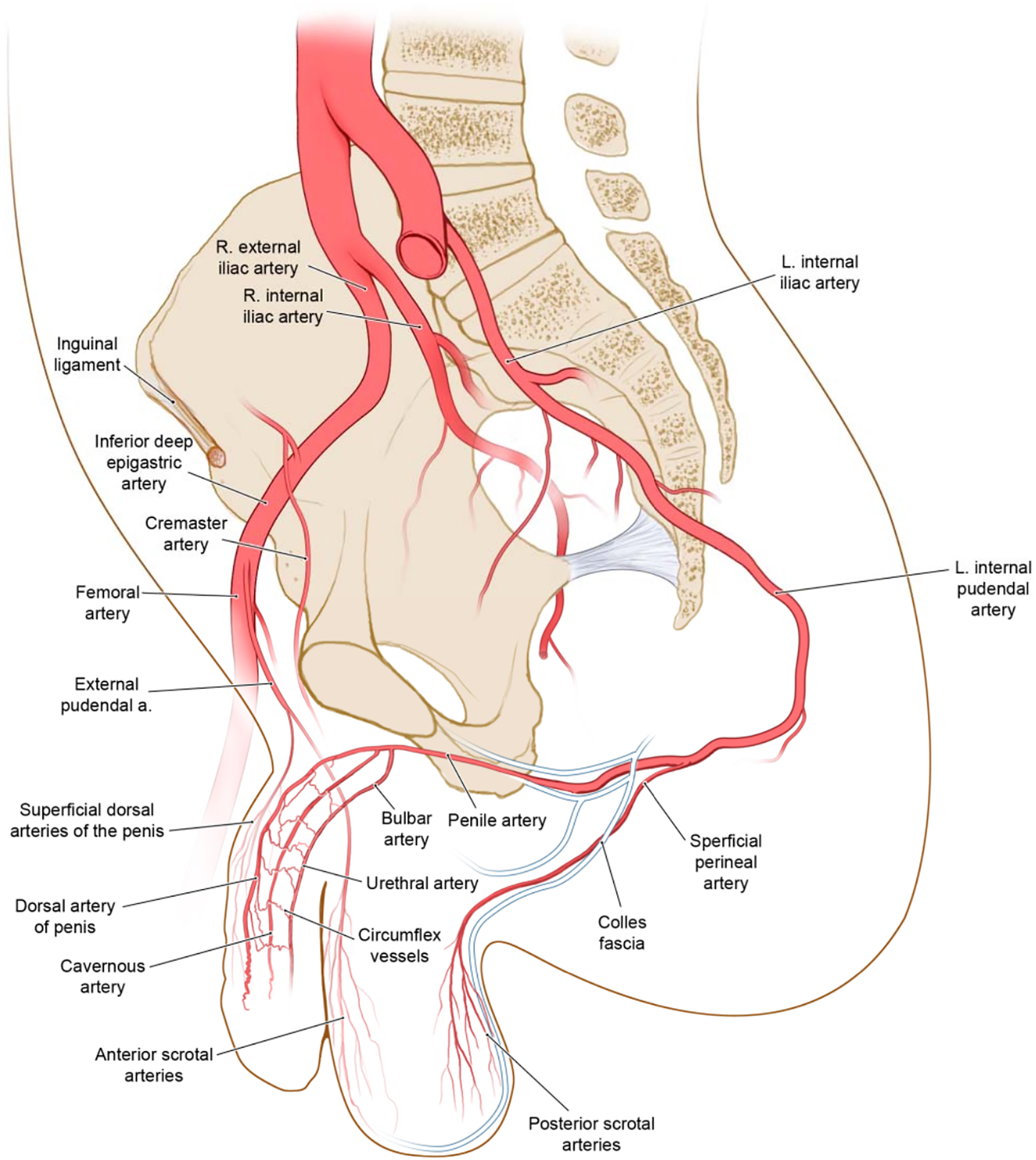
Venous blood is drained from the penis by paired veins. The deep dorsal vein of the penis drains blood from the cavernous spaces into the prostatic venous plexus. Superficial structures of the penis, such as the skin and subcutaneous tissues, are drained by the superficial dorsal veins [ , ].
The scrotum is supplied by the anterior scrotal artery, which originates from the external pudendal artery, and the posterior scrotal artery, which originates from the internal pudendal artery. The scrotum is drained by corresponding scrotal veins that follow the major arteries and drain into the external pudendal vein. These veins and arteries form rich anastomoses and subcutaneous plexuses.
Nerve supply of male genitalia
The nerve supply of the male genitalia is responsible for sympathetic, parasympathetic, sensory, and physiologic reflexes.
The penis is supplied primarily by S2-S4 spinal segments, which pass through the pelvic splanchnic nerves, and spinal ganglia, which pass through the pudendal nerves. Sensory and sympathetic innervation of the penis is supplied by the dorsal nerve of the penis, which is the terminal branch of the pudendal nerve [ ]. This nerve runs along the dorsum of the penis with the dorsal artery, also supplying the skin and the glans. The base of the penis receives its sensory and sympathetic innervation from the ilioinguinal nerve [ ]. Parasympathetic innervation of the penis is from the cavernous nerves from the periprostatic nerve plexus. This plexus of nerves is responsible for the vascular changes of the helicine arteries that supply the erectile tissue, thus forming an erection [ , ].
Innervation of the scrotum is responsible for sensory innervation and the cremasteric reflex. Four nerves are involved in the cutaneous innervation of the scrotum: genitofemoral, pudendal, posterior femoral cutaneous, and ilioinguinal. The cremaster muscle and anterior/anterolateral scrotum receive their innervation by the genital branch of the genitofemoral nerve. This nerve originates from the L1-L2 segments of the lumbosacral plexus and then travels through the inguinal canal to supply the anterior skin of the scrotum [ ]. The posterior aspect of the scrotum receives its innervation from the posterior scrotal nerves, which are derived from the perineal branches of the pudendal nerve and femoral cutaneous nerve [ ]. The cremasteric reflex is due to a sensory synapse from the ilioinguinal and genitofemoral nerves that activate motor neurons. This physiologic reflex has both protective and thermoregulatory functions [ ].
Function of male genitalia
Many male patients seeking aesthetic surgery are looking to alter their genitalia for personal, and often sexual enhancements, despite having physiologically normal function. Male genitalia serve 2 main physiologic purposes: reproduction and micturition.
One main function of the penis is to drain urine from the body. Urine flows from the bladder, through the bladder neck where it passes the internal urethral sphincter via involuntary parasympathetic control. Urine then passes into the prostatic urethra, through the membranous urethra, and then past the external urethral sphincter into the spongy penile urethra. From there, it goes into the navicular fossa and out of the penis through the external urethral sphincter.
From a reproductive standpoint, the penis and scrotum play important roles in sexual intercourse and thermoregulation, respectively. The scrotum is responsible for keeping the testicles several degrees below the average body temperature, which is essential in sperm production [ ]. For intercourse, the penis gains an erection via engorgement of the corporal bodies through parasympathetic innervation. The erectile tissues of the corpora cavernosa and spongiosum engorge with blood and become firm for penetration, whereas the bulbospongiosus and ischiocavernosus muscles compress the veins and prevent drainage of blood from the corpora. Sympathetic innervation allows for semen to exit the penis during the emission and ejaculation phases. After ejaculation, the penis becomes flaccid again due to sympathetic stimulation, constriction of the coiled helicine arteries, and relaxation of the bulbospongiosus and ischiocavernosus muscles, allowing for blood to drain from the cavernous spaces (see Fig. 4 ) [ ].
Male Genital Enhancement Nonsurgical Procedures
During the past few decades, there have been many surgical advances that have made way for the improvements in the appearance and enhancement of male genitalia. Surgical advances have largely centered around penile lengthening, scrotal reduction, and the correction of the hidden or buried penis but there have also been nonsurgical advances that focus on girth enhancement and shaft enlargement through the use of fillers and penile extenders [ ]. This section will focus on nonsurgical male genital enhancement within each section of the male genitalia including the off-label usage of some of these enhancement procedures.
Liquid injectable silicone (LIS) for cosmetic use was first used in Japan, Germany, and Switzerland in the 1940s. It obtained Food and Drug Administration (FDA) approval in 1960s and in the 1976 it was criminalized. The first report of LIS use for penile augmentation was in 1973, which resulted in lipogranuloma [ ]. Although LIS injection has demonstrated effectiveness for various specific purposes, its safety and effectiveness in the context of penile girth enhancement remain unclear. Therefore, we do not encourage its usage for penile enhancement because foreign body reaction is inevitable and can result in disastrous complications that require treatment, which is not only difficult to obtain but also may lead to significant morbidity.
Hyaluronic acid (HA) is a durable and bioabsorbable dermal filler, which is safe, including FDA approval in multiple variations. In a study involving 41 men who received HA injections for penile girth enhancement, the treatment resulted in a significant increase in midshaft penile circumference, from 7.48 cm to 11.4 cm at 1 month and 11.26 cm at 18 months. However, patient satisfaction declined from month 1 to month 18, likely due to a reduction in erectile rigidity and decreased tactile sensation in the shaft, as the corpora cavernosa became covered with softer HA. Despite these negative effects on sexual function, no deformities, inflammation, or adverse events were reported [ ]. In contrast, other reports have associated HA injections with severe complications such as arterial embolization and hypersensitivity but these complications have not been observed in the context of penile HA injections. If used, strict postoperative protocols should be followed to maintain its longevity, which is limited due to the product.
Polymethyl-methacrylate (PMMA) microspheres have also been studied for penile augmentation. PMMA is a nonabsorbable soft tissue filler. The microspheres, when injected subcutaneously, are encapsulated into granulation tissue after which collagen and vascular tissue can embed the microspheres. Casavantes conducted a retrospective 8-year study involving successive PMMA injections to enhance penile girth. They conducted 1500 injection procedures on 729 men, including a significant portion of patients who had previously undergone different girth enhancement treatments. Penile girth increase an average of 2.4 cm and flaccid length of 0.7 cm. About 52% of patients experienced nodularity, ridges, irregularity, indentations, or voids of tissue filler. [ ] We do not encourage the use of this foreign body filler for phallus enhancement due to the high risk of complications that may result from its use and the difficulties in its treatment.
Glans penis
Although most male genital aesthetic enhancement techniques tend to focus on girth and length, there exists a subset of patients who desire augmentation of the glans penis and those who are unhappy with the level of glans tumescence observed during an erection [ ]. One such way that this issue has been addressed is through the implementation of injectable filler and/or the use of implantable grafts and fillers. HA gel has been found to be a suitable and the most ideal injectable for glans penis augmentation because it offers good biocompatibility, is cost-effective, long-lasting, and does not tend to cause hypersensitivity reactions [ , ]. It also can be easily injected using a linear threading or fanning technique but is not widely used due to concerns of the patient possibly developing loss of sensation to the penis [ ]. For this reason, it has also been used as a treatment of premature ejaculation.
Scrotum
One newly emerging cosmetic advancement when it comes to the enhancement of the scrotum is the implementation of neurotoxin injections. Some men present with the concern of having a scrotum that seems too wrinkled, small, or low hanging. Although its usage for the enhancement of male genitalia is considered off-label, new studies have shown that the use of Botulinum Toxin A can help correct bromhidrosis, the appearance of scrotal wrinkles, and help the scrotum seem larger [ ]. The effects have been noted to take 3 to 15 days before results are visibly seen but, overall, patients report satisfaction with the smoother appearance of the testicles and increase in perceived size [ ]. These studies are fairly new and have not fully been tested for the effects on male fertility but they prove promising for men who no longer desire progeny.
Penile shaft
Although many men fall within the normal penile range, there still exists a large subset of men who are dissatisfied with the size and appearance of their penile shaft [ , ]. For lengthening of the penile shaft, nonsurgical approaches have included stretching devices and the use of penile weights [ ]. Penile stretching devices have been shown to increase penile length by 0.5 cm but must be worn by the patient multiple hours each day to achieve said effects [ ].
When it comes to overall satisfaction with the penile shaft, girth has been noted to be more important in the area of sexual satisfaction [ ]. Our efforts at modification of the phallus have been more effective in girth versus length. The most popular of these nonsurgical procedures include the injection of synthetic materials, with the most common being liquid silicone and HA [ ]. Whereas we do not advise injection of nonabsorbable filler materials for phallus augmentation.
Treatment of Complications Resulting from Male Enhancement Nonsurgical Procedures
Although the desire for length and girth enhancement of male genitalia has led to recent developments in nonsurgical augmentation procedures using injections, such as silicone and HA, these do not come without their share of complications. The surgical option of fat injections has shown some success in the enhancement of penile girth; however, we have seen dermal fat grafts work better in these augmentation cases.
Complications that can develop from the use of fillers into penile tissue include tissue ischemia from too large or superficial injections and foreign body granulomatous reactions. This complication can be managed by treating the area with hyaluronidase if HA was used, gentle massage, heat packs, topical nitroglycerine paste application, anti-inflammatory medications, and oral steroids to manage the inflammatory process before more aggressive maneuvers such as surgical intervention for the removal of material and reconstruction [ ].
The use of silicone within the penis can cause a severe inflammatory response, which can lead to deformities such as ulcerations resulting from extrusion of the material through the skin by the body rejecting the foreign body. The way the host’s body reacts to silicone injection can differ but it is commonly associated with the presence of multinucleated giant cells, the accumulation of collagen around pseudocystic vacuoles by fibroblasts, and the possible blockage of nearby microvessels, which can be seen on radiographic imaging. Symptomatic reactions to penile LIS (liquid silicone) injection have included significant swelling, distortion of the penis due to silicone granulomas, and sexual dysfunction. These adverse events have been observed even as long as 30 years after the injection. In many cases, patients experiencing these cosmetic and functional issues have needed surgical removal and reconstruction ( Figs. 5–9 ) [ ]. Surgical management should only be performed by a very experienced surgeon in this anatomic region because risks to the urinary tract, vascular supply, sensory innervation are high, and the reconstruction involves the use of local and regional flaps, which are not commonly performed.

Related posts:
 Nonsurgical Approach for Neck Rejuvenation
Nonsurgical Approach for Neck Rejuvenation
 Cannula Versus Needle for Rejuvenation of the Perioribital Region
Cannula Versus Needle for Rejuvenation of the Perioribital Region
 Modified (Scarless) Orbital Decompression Technique
Modified (Scarless) Orbital Decompression Technique
 Brow Lifts in Male Patients
Brow Lifts in Male Patients
 Update on Three-Dimensional Imaging Technologies and Their Impact and Use in Cosmetic Surgery
Update on Three-Dimensional Imaging Technologies and Their Impact and Use in Cosmetic Surgery
 Advancements in Plastic Surgery
Advancements in Plastic Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


