Introduction
The surgical management of adult brachial plexus injury (A-BPI) reconstruction has evolved substantially over the last century. The advancement of the operative microscope and surgical loupe magnification, micro-instruments and stitches, nerve stimulators, chemistry, molecular biology, and pharmacology has enabled a far deeper understanding of the internal anatomy of the nerves and pathophysiology of nerve degeneration and regeneration. As a result of more accurate preoperative diagnosis, microsurgical skills, more nerve transfers, and functioning free muscle transplantation (FFMT), significant improvements in the functional outcomes of brachial plexus reconstruction have been achieved consistently, since 1970. Nevertheless, there are still many questions with few answers, and many debates with few conclusions. One of the major stumbling blocks to clarity is the lack of general consensus, due to inadequate communication and collaboration.
Many reconstructive surgeons are interested in brachial plexus reconstruction but they feel frustrated due to its complexity ( Box 21.1 ). This author has handled more than 1800 cases of adult brachial plexus exploration and reconstruction since 1985. The aim of this chapter is to give a comprehensive overview of this experience and to make the subject more accessible, with the further goal of obtaining a more general consensus for A-BPI reconstruction.
- 1.
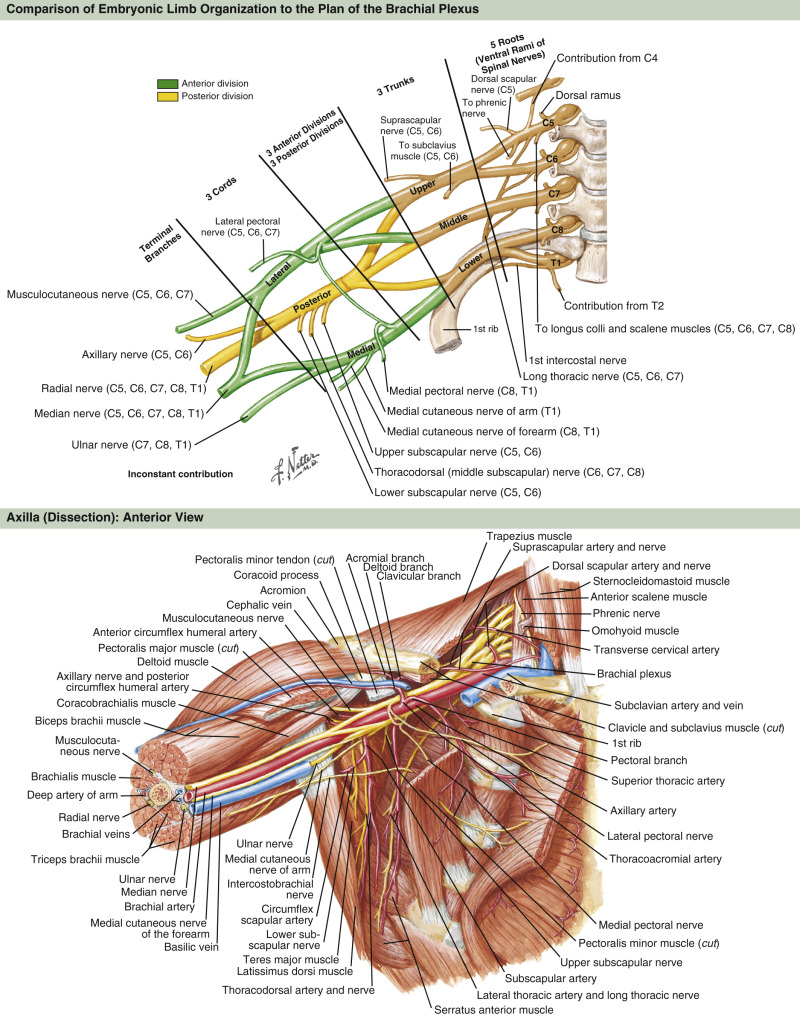
Complex and confusing anatomy
- 2.
Complex pathophysiology (nerve de- and regeneration)
- 3.
Complex evaluation (physical examination and diagnosis)
- 4.
Complex surgical techniques: microneurovascular surgery
- 5.
Long rehabilitation and long follow-up period
- 6.
Different palliative surgeries for sequelae deformities
- 7.
Unpredictable BPI reconstruction outcomes
Consensus in Levels of Adult Brachial Plexus Injury
Different pioneers have had quite varied ways of describing levels of A-BPI. Numerous classification systems have made the anatomy of the brachial plexus more confusing than it need be. A simple and easy classification system has been developed by the author. This system simply uses numbers (I–IV) for the levels of A-BPI ( Fig. 21.1 ) based on key points of the surgical approach:
- •
Level I injury: an injury inside the (vertebrae) bone, basically a preganglionic root injury involving cord, rootlets, or roots. A laminectomy is required for nerve exploration. The incidence of Level I injury is, unfortunately, the highest, around 70%.
- •
Level II injury: an injury inside the (scalene anterior and middle) muscles, equal to a postganglionic spinal nerve injury. Segmental resection of the anterior scalene muscle is required for nerve exploration. The incidence of pure Level II injury is about 8%.
- •
Level III injury: an injury in the pre- and subclavicular space, equal to a trunks and divisions injury. Osteotomy of the clavicle is usually required for nerve exploration. The incidence of pure Level III injury is about 5%.
- •
Level IV injury: an injury in the infraclavicular space, equals to a cords and terminal branches injury. It usually requires tedious dissection and long nerve grafts. The incidence of pure Level IV injury is about 17%, the second highest.
The use of this “number” description for levels of BPI has now been uniformly applied in the author’s center.
Management of Adult Brachial Plexus Injury
Management of A-BPI, using the author’s modified classification system follows. Avulsion and rupture are the two types of lesion frequently seen in A-BPI. Both are traction injuries but with different characteristics ( Table 21.1 ). Root avulsion in BPI is usually accompanied with tearing of the dura and a CSF leak with cyst formation, known as a “pseudomeningocele.” In some cases, the root can be avulsed at its origin with an intact dural cone and no cyst formation. This is called “avulsion in situ,” which gives a grossly normal appearance but with some loosening and/or curvature of the involved spinal nerve at the time of surgical intervention, despite established paralysis. Most often, the entire avulsed roots, including the ventral and dorsal roots and the ganglia, retract and migrate downward to the interscalene or preclavicular region. Clinically, C5 tends to be ruptured, C7 and C8 avulsed, but T1 stretched in injury patterns.
| Avulsion | Rupture |
|---|---|
| Nerve torn from its attachment or at the bone margin | Nerve division + traction: nerve deficit, nerve gap or neuroma incontinuity |
| In the operated field, only one disrupted end can be found | In the operative field, two disrupted ends can be found |
| It may be: | Level II, III, or IV lesions |
| Proximal avulsion: Level I nerve avulsion from the cord or root | |
| or | |
| Distal avulsion: Level IV injury, nerve avulsion from the muscle or at the bone margin |
Consensus in Timing of Brachial Plexus Exploration
Early nerve surgery (immediate or within weeks); delayed early nerve surgery (3 weeks to 6 months); and late nerve surgery (>6 months after injury), are three generally accepted time periods for nerve exploration. Timing of nerve exploration is dependent on the degree of nerve injury. Degree of peripheral nerve injury can be classified into Sunderland grade 1–5 injury. In Sunderland 4° or 5° injuries, only nerve repair can succeed in restoring continuity. In Sunderland 1°, 2°, and 3° injuries, spontaneous recovery may occur. In cases of penetrating injury by sharp objects in A-BPI, it is clear that early nerve surgery is indicated. For a closed traction injury, some surgeons advocate early nerve surgery. This is much debated in Level IV injury because of the desire to avoid tedious scar dissection and long nerve grafts. However, most brachial plexus surgeons recommend delayed early nerve surgery for closed type of A-BPI, no matter which level of injury. The reason is that in closed BPI with avulsed or ruptured stumps, it is often difficult to judge the degree and extent of injury so soon after trauma. The use of healthy stumps is more crucial for better outcomes. In such cases, the benefits of waiting outweigh the advantages of early nerve surgery.
Clinical Presentation and Examination
Patient History
A-BPI may be caused by trauma sustained in motorcycle accidents (the most common cause; about 80%), falling from a height; traction injuries from rolling machines or conveyer belts; compression injuries from heavy objects or shoulder dislocation; penetrating injuries from sharp objects or bullets; iatrogenic injuries; or even those from surgeons during tumor resection. Other causes are tumors (primary or secondary), infections (e.g., enterovirus, polio), or inflammation (e.g., irradiation neuritis).
Patient history helps to classify the degree and extent of injury. A history of shoulder dislocation or glenoid fracture may show a high incidence of Level IV injury. A history of C-spine fracture indicates that Level I root injury is more likely. Artery rupture and repair can help determine the site of nerve injury based on level. Segmental thrombosis of the subclavian artery is usually associated with C8 T1 Level I root injury. History of rib fracture and chest intubation warns against intercostal nerve transfer because of higher failure rate. Limping due to lower limb fracture with osteomyelitis or non-union will also affect the intercostal nerve transfer as the patient will not be able to perform appropriate rehabilitation. Extreme causalgia, often seen in cases with root avulsion in aged patients, is also a major risk factor for poor results due to poor rehabilitation.
Patient Examination
Patient examination is essential and is the most important step in establishing the diagnosis of the site and degree of injury. The patient is examined initially and again at 2 months post-injury, in order to get an accurate assessment of the level and degree of injury.
Motor Examination
Motor examination should be completed, muscle by muscle, in a disto-proximal fashion, and recorded using the British MRC (Medical Research Council) scale (M0–M5), which gives each muscle a level of strength, with M0 having no movement and M5 having normal contraction against full resistance.
Sensory Examination
Sensory evaluation should include a pinprick pain test and Tinel sign. A pinprick test from areas of normal to abnormal sensation will map out the area of sensory disturbance and is sufficient for the patient’s sensory examination. Sensory grading is based on the British MRC scale (S0–S4), modified by adding a grade for sensory over-reaction (S2+). Such sensory evaluations can give clues about the level and degree of brachial plexus injury. Tinel’s sign is an important clinical way to determine the location of neuroma or to judge the regeneration of the injured nerves. Palpation or percussion at the neck, at the supraclavicular Erb’s point (clavicular insertion of the sternocleidomastoid muscle), at the infraclavicular coracoid process of the scapula, and at routes of different nerves pathways may induce electric current sensation (like pins and needles) running down to the shoulder or the hand. This is called “positive Tinel’s sign.” Tinel’s sign should be localized at the point of maximal pain elicited. If the Tinel’s sign remains at a fixed point, implying retardation of nerve growth, surgical exploration is warranted. If the Tinel’s sign advances from supraclavicular to infraclavicular and further to arm or forearm at successive examination, “wait and see” in this instance is recommended. A weak or absent Tinel’s sign in the neck region with a paralyzed limb usually indicates a total root avulsion. Horner’s syndrome (miosis, ptosis, enophthalmos and anhidrosis) is a sign of sympathetic nervous system disturbance. It indirectly implies avulsion of T1 and C8 roots. This syndrome usually persists in A-BPI.
Vascular Injury Examination
Absence or weakness of pulsation of the radial artery at the wrist indicates vascular injury of the axillary or subclavian artery. Vascular injury should be taken into account when considering the use of a vascularized ulnar nerve graft for reconstruction. FFMT for reconstruction should also be very carefully used in cases of absence of radial artery pulsation. Splint immobilization that keeps the elbow in flexion at more than 90° can easily compromise digital peripheral circulation.
Root Injury Pain
Brachial plexus root pain is caused by avulsed nerve stump wound (acute stage), or healed scars (chronic stage) with pain. It is similar to a wound (acute stage) or healed scar (chronic stage) on the skin. The skin wound scar may cause itching and tingling pain on the skin, but regresses from time to time. Brachial plexus root pain was similar, beginning with severe and frequent nerve shooting pain, to the intermittent but regressive pain. But sometimes it may persist indefinitely if the nerve stump was healed by bad scars. Typically the root pain will have no precise distribution and is described as an electric shooting pain continuing for short duration (seconds), resolving spontaneously and recurring. This characteristic pain is called “deafferentation pain.” The pain can be induced by temperature change, but relieved by psychological pathways such as the distraction mechanism (concentrating on other tasks such as working, exercise, gardening, change of posture, massage). This distraction of pain is very helpful and should be well explained with the patient and patients’ family. The best treatment for root pain is distraction, rather than medicine or surgery.
Plain X-Ray and Imaging Studies (MRI and/or CT)
Plain X-rays of the chest and cervical spine are routinely required. Chest X-rays should include inspiration and expiration views to exclude diaphragmatic palsy. C-spine X-rays are evaluated for any fracture of the transverse or spinous process as well as the vertebrae body. Cervical scoliosis or neck spine rigidity is a possible sequel of Level I injury.
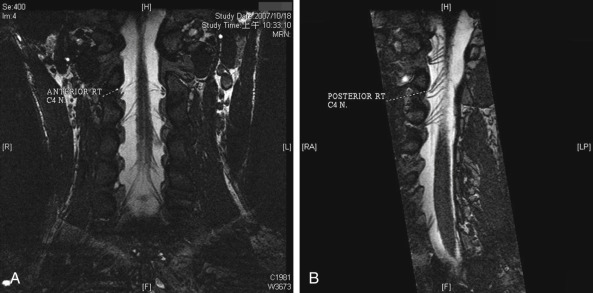
In recent years, invasive imaging studies (such as cervical myelography) are gradually being replaced by non-invasive magnetic resonance imaging (CT-myelogram and 3D-MRI). An MRI study with various investigative techniques is very helpful for diagnosis of root injury. Improved techniques for diagnosis include C-spine MRI myelogram; 3D-FIESTA (Fast Imaging Employing Steady-state Acquisition) study provides rapidly obtained images of fluid-filled structures with continuous slices from the antero-posterior cutting plane ( Fig. 21.2 ), different planes of ventral and dorsal rootlets using curve planar reformat technique; MRI, diffusion weighted imaging (DWI), and short tau inversion recovery (STIR) techniques with views of the Level II–IV nerve structures. Valuable and accurate data provided by the various MRI techniques allow surgeons to make more confident judgments on the level injury of A-BPI.
Electrodiagnosis
Electrodiagnostic studies, mainly consisting of nerve conduction velocity (NCV) and needle electromyography (EMG), are used to localize the lesion and to assess its severity. Abnormal low sensory action potential (SNAP) amplitude indicates a ganglionic or post-ganglionic lesion. Conversely, the pick-up sensory action potentials taken from a paralytic limb is evidence of a Level I lesion. The presence of fibrillation potentials on needle EMG may suggest that the lesion is at least axonotmesis. The significant reduction of the amplitude of compound muscle action potentials during motor nerve conduction studies indicates an axonal loss (Sunderland 3–5° lesion), rather than a neurapraxia (Sunderland 1°) lesion.
Surgical Treatment
Nerve surgery is always the treatment of choice for A-BPI, whether that be for closed or open injuries. For closed BPI, management can be considered in the six stages:
- •
Stage 1: Stabilization stage (the 1st month), including stabilization of vital signs, bone fracture, or joint dislocation
- •
Stage 2: Diagnostic stage (the 2nd month), including clinical examination and ancillary investigations to establish the diagnosis of the lesion condition; start of physiotherapy to prevent soft tissue swelling, joint stiffness, slow muscle atrophy by electric stimulation; and psychologic education before surgery
- •
Stage 3: Nerve surgery (the 3rd to 5th month): if the patient fails to show a return of function at 5 months, surgical intervention is indicated. Nerve reconstruction with nerve grafts or nerve transfers at 5 months seems to make no big difference, with surgery in the 3rd month in results of our series. However, results of nerve reconstruction performed more than 6 months after injury are usually significantly poorer than the denervation time of less than 6 months. Therefore, waiting until later than 6 months after injury to perform nerve grafts or nerve transfers is not recommended and often local or free muscle transfers might become necessary to enhance the results
- •
Stage 4: postoperative care (3–4 weeks postoperatively) and rehabilitation (3–4 years)
- •
Stage 5: late reconstruction for the sequelae deformities or deficits (during 3rd or 4th year postoperatively)
- •
Stage 6: destination stage (5th or 6th year postoperatively) including amputation and intolerable pain treatment.
In chronic cases (1 year after injury), the muscles have undergone long-time denervation and atrophy, so late nerve surgery in such circumstances is useless and usually leads to poor results. FFMT, or banked nerve grafts from ipsilateral or contralateral nerve transfer followed by secondary FFMT is the option for such chronic cases.
Exploration of the Supraclavicular Brachial Plexus
A C-curved incision – starting midway along the posterior border of the sternocleidomastoid muscle down to 6–8 cm, and curving laterally parallel to and above the clavicle to a point to connect the line of deltoid-pectoral sulcus – is a popular incision for supraclavicular approach ( Fig. 21.3 ). A platysma musculocutaneous flap is elevated. Dissection beneath the sternocleidomastoid muscle is made to the internal jugular vein, a landmark of the uppermost medial dissection. The supraclavicular sensory nerves are the landmarks of the uppermost cranial dissection. The omohyoid muscle traverses just behind the sternocleidomastoid muscle and is looped and spared, as it can serve as an important landmark if a secondary surgery is necessary (deep to the plane of this muscle are more critical structures including the brachial plexus). Below the omohyoid muscle, there is an abundance of adipofascial tissue containing rich lymphatic duct and lymph nodes. The transverse cervical vessels also exist in this space. A similar C-shaped incision along the internal jugular vein medially and subclavian vein inferiorly is made and a superiorly based adipofascial flap is elevated. The lymph tissues, including the ducts coming from the deep plane of the internal jugular vein, should be coagulated or ligated before division to avoid postoperative lymph leakage and chylous formation. The transverse cervical artery and vein in the deeper plane of the adipofascial tissue are preserved if possible, as they may potentially be required as recipient vessels for a vascularized ulnar nerve graft. Following the elevation of the adipofascial flap, the phrenic nerve is noted over the scalene anterior muscle. The subclavian artery lies just beneath the scalene anterior muscle and inferior to the C7 spinal nerve and should be carefully protected. The dominant transverse process of C5 at the top of the supraclavicular sensory nerves is palpable. If necessary, the fibrotic scalene anterior muscle attached to the C5 transverse process can be detached and segmentally excised to expose the C5 and C6 spinal nerves: the spinal nerve above the C5 transverse process is C5, and below is the C6 spinal nerve. The C7 spinal nerve is usually located a little farther away from C6. C8 and T1 spinal nerves or of the inferior trunk are then noted deep beneath the subclavian artery. Sometimes the C8 is quite close or adherent to the C7.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


