Zouboulis CC, Fischer TC, Wohlrab J, Barnard J, Alió AB. Cutis 2009; 84: 223–9.
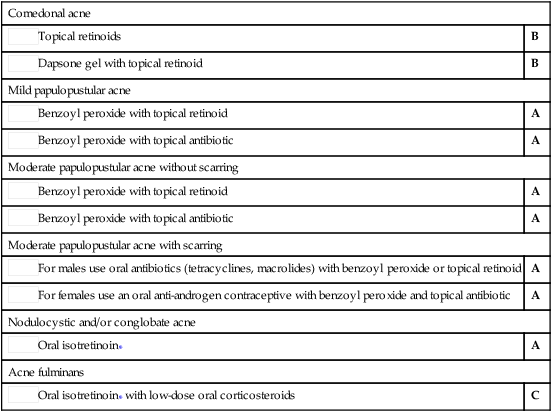
Acne vulgaris

First-line therapy
Comedonal acne
 Topical retinoids
Topical retinoids
B
 Dapsone gel with topical retinoid
Dapsone gel with topical retinoid
B
Mild papulopustular acne
 Benzoyl peroxide with topical retinoid
Benzoyl peroxide with topical retinoid
A
 Benzoyl peroxide with topical antibiotic
Benzoyl peroxide with topical antibiotic
A
Moderate papulopustular acne without scarring
 Benzoyl peroxide with topical retinoid
Benzoyl peroxide with topical retinoid
A
 Benzoyl peroxide with topical antibiotic
Benzoyl peroxide with topical antibiotic
A
Moderate papulopustular acne with scarring
 For males use oral antibiotics (tetracyclines, macrolides) with benzoyl peroxide or topical retinoid
For males use oral antibiotics (tetracyclines, macrolides) with benzoyl peroxide or topical retinoid
A
 For females use an oral anti-androgen contraceptive with benzoyl peroxide and topical antibiotic
For females use an oral anti-androgen contraceptive with benzoyl peroxide and topical antibiotic
A
Nodulocystic and/or conglobate acne
 Oral isotretinoin*
Oral isotretinoin*
A
Acne fulminans
 Oral isotretinoin* with low-dose oral corticosteroids
Oral isotretinoin* with low-dose oral corticosteroids
C
Study of the efficacy, tolerability, and safety of 2 fixed-dose combination gels in the management of acne vulgaris.
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree