CHAPTER 4 A Comprehensive Evaluation of the Cosmetic Oculoplastic Surgery Patient
Beyond Formal Measurements. Decision Making and Tips to Enhance Patient Satisfaction and Outcomes
The accurate evaluation of the patient who presents for consideration of aesthetic improvement of the periorbita is as important as any of the other components that lead to a successful outcome. Often an unfavorable result can be traced back to a less than precise evaluation of the situation at hand that would include failure to observe some of the salient findings that were neither protected or improved. Frequently patients present with a general dissatisfaction of the aging appearance of the periorbita, but are not quite exactly sure what are the particulars that bother them, the options for improvement, or the potential risks with the multitude of approaches. As in all aspects of medicine, an accurate history, physical examination, and thorough discussion with the patient will lend itself to better treatment planning. This combined with precise surgical execution, will nearly always result in a happier patient. More often, even subtle findings or clues that lend themselves to particular maneuvers that will optimize the overall result can be seen before (or are seen retrospectively) by careful evaluation of the patient and review of preoperative photographs. In this chapter, I will discuss some of the important aspects of this process, including choices and decision making that must be considered in every patient evaluation for the individual who presents for periorbital cosmetic surgery.
History
The patient’s purpose for their consultation and general history is commonly first obtained by a nurse, medical assistant, or resident/fellow in training. At times this is obtained only and directly by the surgeon him/herself. If the initial history is taken by someone other than the operating surgeon, it behooves the surgeon to review the obtained data and often supplement the historical information with data that will improve and clarify the overall patient status. This starts, as with all medical evaluations, with a chief complaint. Sometimes the chief complaint is disregarded only to be discovered after surgery when the patient states that although there is obvious improvement of the overall presenting condition, the main purpose for this patient proceeding with surgery was to improve a situation that was clearly stated in the chief complaint and possibly forgotten, ignored or not adequately addressed in the final analysis. Obviously, once the patient makes this statement, their expectations are that this will be addressed, despite the elaboration and performance of other procedures that might globally improve the appearance of the periorbita and face. These additional procedures are usually recommended after either an expanded description of the chief complaint, or by questions asked directly by the medical assistant or physician which further clarify the situation and are then a prelude to a more meaningful discussion of this and the potential options for their remedy.
History of allergies to medications as well as other known substances (including latex, injectable anesthetics, etc.) should be discussed. For instance, patients will often state that they are ‘allergic to lidocaine’ and when on further elaboration they claim that asymptomatic palpitations were noted during a dental procedure, for example. Often they will consider this an allergy or contraindication to use, when in fact under controlled and monitored anesthesia this may not be the case. If they claim an allergy to a particular drug, they should also describe (if they can recall) exactly what type of ‘reaction’ occurred during the usage of this medication or drug. Commonly patients will state other (non-allergic) symptoms including ‘upset stomach,’ nausea, lethargy or sleeplessness, all of which are obviously not necessarily true allergic responses. Patients should be directly questioned on the use of any anti-inflammatory medication or any drugs which could potentially increase bleeding time; this medication will probably be discontinued for at least one to two weeks prior to surgery. A list of medications that could alter bleeding times may be given to them for a review and reminder. They should also be questioned regarding personal experiences with bruising or bleeding which may help counsel patients on what they can expect regarding their appearance immediately after surgery.
Finally, a history of dry eye symptoms, use of artificial tears and other topical emollients for the eye surface, as well as the use of contact lenses should be elicited that may give you more information than can be obtained by didactic measurements.1,2 For instance, if a patient states that they have intermittent dry eye symptoms of irritation, pain, light sensitivity, and decreased vision, an elaboration of these questions may reveal that the patient infrequently uses tear supplements and by increasing their usage of the topical agents dramatically reduces and even eliminates symptoms. These patients must be approached (i.e. for surgical candidacy) with great caution and the procedures may be modified to reduce the chance of increased ocular exposure symptoms. Similarly, if the patient states that their dry eyes are ‘terrible’ but also denies the use of tear supplements, or that they are able to tolerate contact lenses for days and weeks at a time without symptoms of dryness or irritation, they can do very well after surgery with regard to the concerns of potentially worsening dry eye symptoms. To the contrary, if a patient denies a history of dry eye symptoms but after further questioning reveals a complete intolerance to the use of contact lenses (due to pain and discomfort), can’t tolerate a fan or air-conditioning (i.e. in a car or plane) blowing near them due to enhanced ocular foreign body sensation, they may pose significant risk when proceeding with any eyelid surgery. Finally, women that are nearing menopause, immediately pre-, or postmenopause, should be warned that their incidence of dry eye symptoms can be worsened even when surgery is performed very well. As this is a common age for women to have cosmetic blepharoplasty, their increased symptomatology is often blamed on the surgery. Appropriate preoperative counseling lets them know that their worsening of symptoms may be expected and fortunately, is temporary in most situations. Finally, those individuals who have had keratorefractive surgery (i.e. LASIK and related procedures), clearly exhibit a greater risk and incidence of dry eye symptomatology after surgery, and this should be discussed beforehand, so that the choice to proceed with cosmetic blepharoplasty, understanding the risks, becomes theirs.
The physical examination
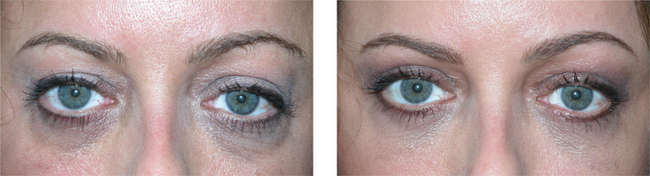
The first part of the physical examination begins during the history taking process. I commonly will simply observe a patient while they are speaking, and simultaneously evaluate them for animation and effects that may relate to either their complaints or possibly recommendations and treatment options. Asymmetries are commonly noted, especially with regard to the position of the eyebrow(s), as well as the size of the horizontal and vertical palpebral apertures (Fig. 4-1). At times during this discussion, even subtle facial weakness or dyskinesis can be identified which must be considered while entertaining surgical options, as well as documentation of its presence as it may only become obvious to the patient after surgery. A prelude to the patient’s personality can also at times be detected by their habits and mannerisms. Those who are shy or even untruthful will not as frequently maintain eye contact. Those who continuously question or even argue every statement or recommendation negatively, may cause trouble after surgery even if it is performed at or near perfection. Those patients who have been unhappy with all prior experiences and speak unfavorably about many or all prior treating physicians are also likely to be dissatisfied with your efforts. So the history portion of the consultation is not simply performed to obtain routine historical data, but the treating surgeon should be keenly observant of facial expression as well as personality and mannerism traits of the individual which will lead to the best possible treatment recommendations, that might include no treatment at all.
General upper facial assessment
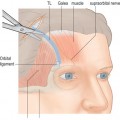
Once the general assessment and more casual observation (during the history-taking portion) of the patient’s situation has been obtained, a more detailed evaluation should follow, including more formal measurements and notations (see Chapter 3) of the eyebrow position and asymmetry. There should be careful evaluation of forehead and periorbital lines and furrows, which will often indicate chronic and habitual animation (Figs 4-2 to 4-5). I do not believe that formal or precise brow measurements will dictate whether or not to perform brow surgery (Fig. 4-6); however it will serve as a basis for discussion of the possible options. For instance, I will often request to review old photographs of the patient to determine their opinion on their brow position in the past and present, and then will discuss the reality of actual brow descent. Photographs are generally helpful for many aspects of periorbital surgery (see Chapter 2), especially in lieu of asymmetry and general aesthetic appearance and ultimately the goal for our rejuvenative efforts (Fig. 4-7). Nonetheless, useful didactic measurements including the vertical and horizontal palpebral fissures, margin to reflex distance (MRD1) and lower lid position with regard to shape, retraction, canthal position and lower eyelid laxity should be determined (see Chapter 3). I have not found reliance on snap-back or lower eyelid distraction maneuvers particularly useful as a screening tool for the necessity (or not) for canthpexy/plasty, especially in lieu of my philosophy that most lower lid surgical procedures (except in the very young) require routine, varying degrees of canthal support5 (see Chapter 15). These maneuvers, however, may simply confirm the necessity for lower eyelid/canthal re-enforcement procedures, and vectors for commissure support or repositioning (Fig. 4-8). They may also serve as an illustration (to the patient) of the need for particular ancillary procedures at the surgical setting.
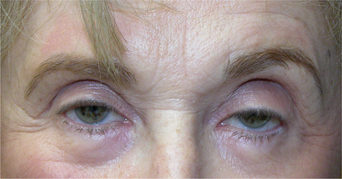
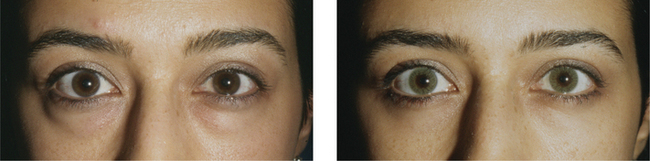
Figure 4-3
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


