9. Male versus Female Facelift Surgery. Is There a Difference?
9.1 Introduction
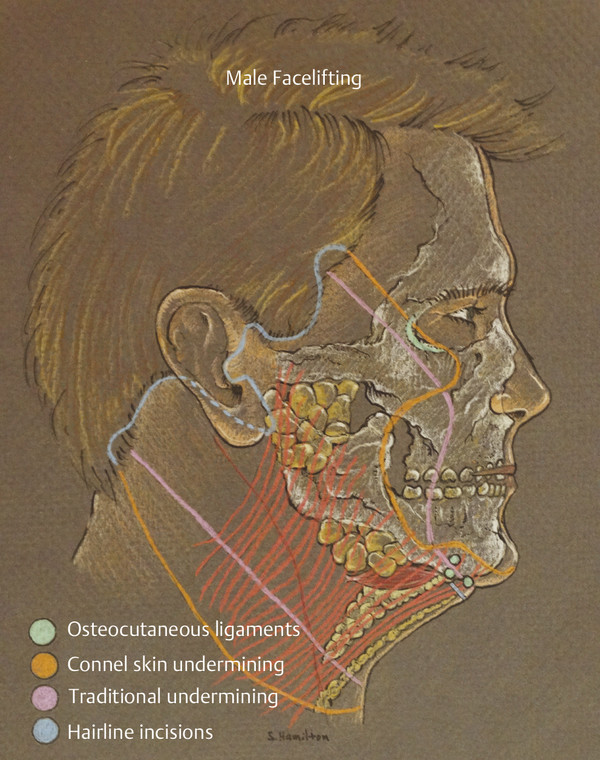
As illustrated in Fig. 9.1, Connell developed a unique set of skills and principles to address male facial aesthetic surgery. As discussed in Chapter 8, the challenges of proper incision design (hairline vs. scalp), bidirectional or lamellar tissue movement of the skin versus the deep tissue, and gender-specific facial proportions form the basis for Connell’s development of a more natural-looking and effective technique for male facial aesthetic surgery. The relative adherence to these guiding principles to generate less obvious scars and more masculine, natural-appearing results forms the bulk of Connell’s legacy of improved facelift results with male patients. Nevertheless, male facelift surgery has remained one of the more ambivalent success stories in aesthetic surgery. A technical “spillover” of classic techniques and principles that restore youthful volume, facial tissue position, and facial aesthetic relationships for women often have been applied directly to male facelift surgery, sometimes with disturbing results. Every year, disturbing “before and after” pictures seem to appear on the Internet involving plastic surgery performed on male public figures in the entertainment, political, and sports worlds that have been transformed into examples of androgynous, often distorted images of men with facelifts that achieve a measure of gender crossover and diminishment of original identity.
The subject of masculinity or femininity is sometimes a touchy subject with patients, as they may harbor biases or misperceptions that call for calm, intuitive exploration and clinical guidance in order to arrive at a suitable gender-friendly outcome.
A fascinating study of female gender perception, sexual attraction, and trust was carried out in England in the 1980s (Fig. 9.2) 1 , 2 that illuminates the perceptual connection between male appearance and perceived masculine attractiveness. The female test subjects were given two photoshopped versions of the same male face and asked to answer parallel interrogatories. One version of the experimental male face was masculinized 50% by photoshop enhancement and notable for a lower brow with a more restive, hooded eye. The jaw was also stronger, more defined in lateral contour, and longer. Lips were not inflated. The second image was an equally feminized version of the same face. The eyebrows were higher with noticeable increase in pretarsal skin show. The jaw was narrower and appeared weaker. Lips and cheeks were fuller.
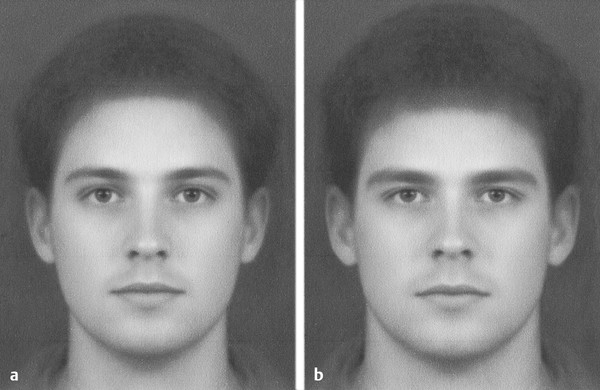
The test subjects overwhelmingly preferred sexually the more masculine version, and presumably, this was the choice for genetic source for procreation. Surprisingly, subjects preferred the feminized version for long-term, trusting, supportive relationships and confidence that the man would be able to assist them in raising offspring. This study not only points out the duality of sexual attraction that strong or weak facial markers of masculinity stimulate, but also implies to the aesthetic surgical community that extreme care is necessary not to imbalance a content, well-adjusted male patient’s life by drastically unbalancing this visceral response by women and peer group alike. It is not our occupation to design or live our patients’ lives, but it should be our general rule never to alter their gender destiny, whatever it may be, without careful discussion and disclosure of alternative outcomes possible that either preserve masculinity or reduce it to design the proportion of change sought by the sometimes defocused male patient. Like women, men do seek rejuvenating surgery, but they lack the casual, often traveled line of reasoning, language, and self-assessment more common to women. It takes careful observation and a degree of empathy to navigate a productive evaluation and surgical plan with a male patient. One simple method to communicating visually with the less-than-perfectly-communicative male patient is to show photographs from magazine ads and articles that portray differing examples of male archetypes. These photos should demonstrate clear differences in brow position, pretarsal skin show, midfacial volume, jaw definition and strength, and lip volume. One finds that patients are more comfortable projecting clearer aesthetic bias on a photo of a stranger than with themselves. Once goals are established, photographs taken of the male patient can then be evaluated for precise differences and changes that may be similarly desired for surgery. So conducted, such interviews can distill core aesthetic goals of the male patients in a more relaxed, nonchallenging manner.
More to the point, had contemporary celebrities been shown similar photographs of men with vacant, overhollowed orbits, arched overelevated brows, displaced hairlines, and overreduced nasal structure, they would likely have chosen alternative procedures.
9.2 Proportion
As in the recommended interview process, evaluation of the differences between male and female facial aesthetics is easily accomplished with side-by-side comparison views of current male and female archetypes. For purposes of discussion, I have chosen Brad Pitt and Angelina Jolie. Both are celebrated for their good looks, and each, in my opinion, shows strong gender tilt to his or her sex. Fig. 9.3 shows a single facial image comprising one-half of each actor. The faces are divided into three levels: upper third, middle third, and lower third. The upper third comprises the brow and eyes to the lid–cheek junction. The middle third is composed of midface, cheek, and nose. The lower third contains the lips, jaw, and upper cervicomental transition zone.
What is immediately obvious is that the greatest proportion of structured, gender-biased differences is located in the upper third of the face. The male brow is lower and unarched. He lacks pretarsal skin show entirely, and his eyelids are full. In contrast, her brow is femininely arched laterally. There is significant pretarsal skin show with deeper, more sculpted upper lid with near absence of orbital fat. The lower eyelid is not overly full. The middle third shows slightly fuller, rounder shape in the female contrasted with the less full, flatter midface of the male. His nose is wider in all areas. The lower third is remarkable for almost exact, parallel aesthetics: defined, clean jawlines and sharp cervicomental transition. The strong, clean jawline seems to be a clear, successful aesthetic crossover feature whether male or female.
Similar evaluation of male–female pairs in magazine ads will confirm, over and over again, this simple breakdown of the divergence of proportion and position of facial aesthetic subunits from the upper to the lower third of the face. Applying this simple finding to facelift surgery remains the task of observant surgeons who strive to restore and enhance their male patients’ facial aesthetics without depriving them of what they are usually seeking: to be a younger version of their aging male appearance.
9.2.1 Upper Third
A quick review of plastic surgery texts showing male blepharoplasty patients will demonstrate the feminizing effect of a marked increase in male pretarsal skin show. Males commonly seek blepharoplasty as their one and only aesthetic procedure. Their conservatism likely reflects that they are either justifiably dubious or simply afraid to delve into further surgical rejuvenation procedures for fear of an artificial surgical look with associated deformity and feminization. Typically, the redundant upper eyelid is due to ptosis of the brow, not to elongation of eyelid skin. Connell has often recommended conservative browlifting in men as a fix for the tired, aging low brow position and to restore the original level of pretarsal skin show seen in early photos of the male patient (Fig. 9.4). It is recommended to avoid increasing the pretarsal skin show in any male patient beyond what they demonstrated in college or early adulthood photographs. In cases of advanced fat herniation, a conservative fat resection with skin preservation accomplished at the time of the browlift will often preserve and restore these early proportions. Delivering more than a 3- to 4-mm pretarsal skin exposure, except in those with genetically high tarsal fold, such as in Mediterranean groups, will often deprive the male upper third of a degree of inherited masculine upper eyelid phenotype.
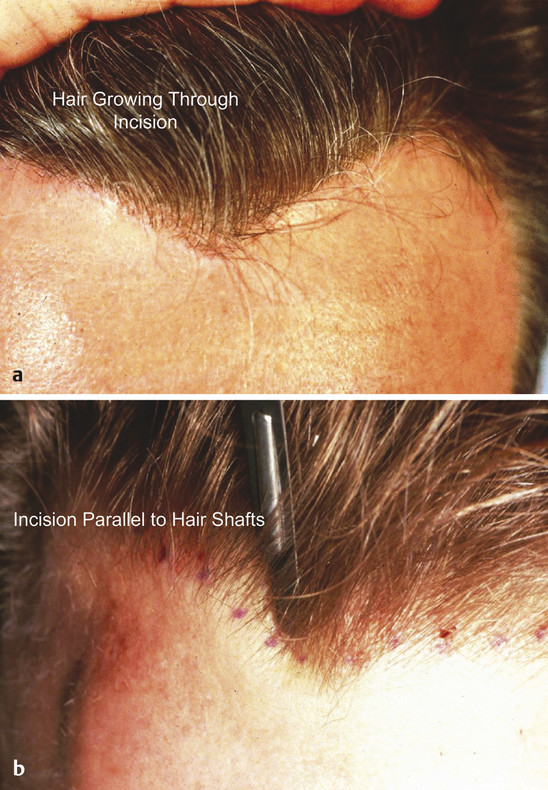
The male brow can be challenging because of high hairline, deep wrinkling, or hypertrophy of glabellar musculature. Reduction of the hairless forehead with a hairline incision is an excellent choice in select patients with a high, overelevated hairline and allows for lowering of the hairline, although low density of hair sometimes drives the choice of technique to alternative open or closed techniques that hide behind the hairline (Fig. 9.5). Hair transplantation can be thought of as an adjunctive camouflage procedure in hairline browlifts with thinning hair; the hairline lift also serves to preserve the bulk of native hair stock.
Care should be taken in approaching the male lower blepharoplasty because excessive fat removal will invariably produce a weaker-looking, depleted, and less masculine eye. Often, laxity of the aging male lid is overlooked and a significant benefit is seen with strengthening the lateral canthus. This also protects against the sometimes typical male postfacelift appearance of sunken, staring eyes with surgically induced mild to moderate ectropion. If hollowing is appreciated at the lid–cheek junction, a facelift with associated midface rotation is indicated, or the patient could be offered conservative fat grafting to restore the depleted orbital appearance as well as to fill deep nasojugal grooves.
An algorithm of correction of the ptotic or atrophied infraorbital region includes orbital fat transposition, facelift with superficial musculoaponeurotic system (SMAS) midface rotation, alloplastic implant, or fat grafting. The latter technique is my choice because it minimizes risk as opposed to more complex open procedures that require disruption of local tissue relationships and attachment. However, as Bruce Connell is fond of saying, any good surgeon can make any alternative surgical technique produce good results. Regardless of surgical bias, a typical plan for aging phenomena should follow a logical, stair-step approach from simple, direct procedures to more layered and complex ones. He believes that surgeries should not follow set patterns or use repetitive “cookbook” solutions to perform generic surgeries such as blepharoplasty, foreheadplasty, or facelifts. Instead, he stresses individualization and precise preoperative anatomical diagnosis of the perceptible aesthetic issues with development of a surgical plan as unique as the patient. With that in mind, training with Dr. Connell could at times be unsettling because he rarely repeated himself technically, and he expected this polymorphic perception to be equally developed in those he trained and quizzed. Early in his career, he used this philosophy to distill unique solutions for male aesthetic surgery, and he published these concepts over the years.
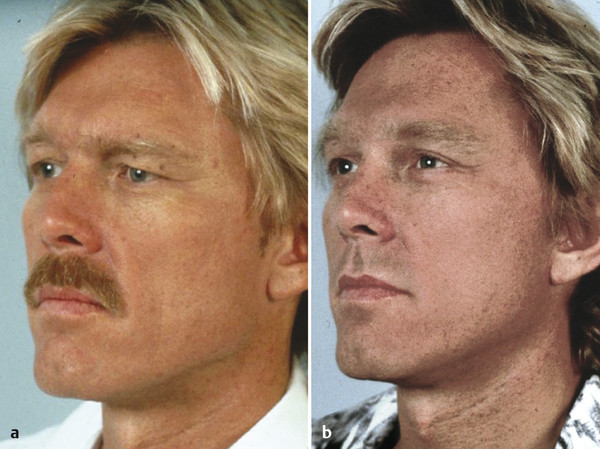
Contrasting examples of upper one-third correction are illustrated in Fig. 9.6. Note that although both male and female patients underwent browlifting and blepharoplasty, the male patient has retained more upper lid hooding and reduced pretarsal skin show compared with the female. The female counterpart shows greater brow elevation and hollowing of the upper lid to accentuate the increased dimension of the pretarsal shelf and increase the overall feminine gender tilt. Both patients have subtle nasojugal and infraorbital hollowing, and both underwent periorbital fat grafting. Note also that the fat graft volume was more aggressive in the female patient to plump the midface slightly, whereas the male simply had the nasojugal fold filled along with more subtle midface filling.
Just as imprudent surgical changes can negatively impact an otherwise gender-appropriate periorbital appearance in either gender, the aging phenomenon can sometimes produce an example of gender reverse engineering. As seen in a comparison of before and after pictures (Fig. 9.6) demonstrating the recommended divergence in periorbital rejuvenation surgery in female versus male patients, the female patient demonstrates severe periorbital atrophy that has transformed her nice youthful, feminine upper facial one-third so that it displays overly masculine qualities. Her superior orbital contour developed an almost 90-degree A-frame deformity while she was in her 50s, seen more commonly in more-advanced-age nursing home populations or in gothic window frames. Note also the small amount of lower lid fat herniation seen in both the male and female patients preoperatively, with marked intraorbital hollowing in the female and deep left nasojugal fold (X) in the male. In both the male and female patient there are deep nasojugal grooves on the left side. The loss and reintegration of feminine gender markers in the woman are demonstrated by comparison of the preoperative and postoperative images. This reintegration was achieved through the use of endoscopic browlift, corrugator debulking, and superior orbital roof and intraorbital fat grafting, along with lower lid blepharoplasty. Her midface was generously fat grafted to achieve slight convexity (Y). Pretarsal height (Z) visibly increased.
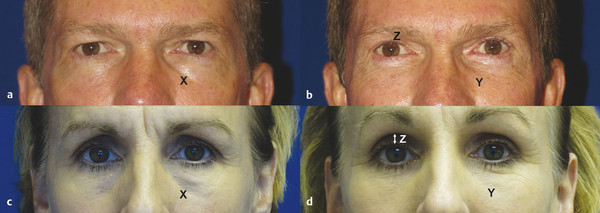
In contrast, (Fig. 9.6 a, b the man) demonstrates brow ptosis, secondary eyelid hooding, lower eyelid fat herniation, and a unilateral left deepened nasojugal fold with mild midfacial volume loss. The corrective surgical algorithm parallels that in the female face except in the degree of correction. The corrective endoscopic browlift maintains a near-zero pretarsal skin height (Z), unlike the increase seen in the female counterpart. Both patients underwent browlift, lower blephasoplasty, and targeted midface fat grafting. The woman had greater volume grafted, whereas the man’s face was kept more hollow (Y).
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


