8 Low Median Nerve Palsy Tendon Transfers
Abstract
The main goal of tendon transfers in the setting of low median nerve palsy is restoration of thumb opposition. Four classic low median nerve palsy tendon transfers exist: extensor indicis pollicis, palmaris longus (PL) (Camitz), flexor digitorum superficialis (FDS), and abductor digiti minimi (ADS) (Huber). Each has a unique set of features and considerations. This chapter describes the preoperative evaluation, intraoperative execution, and postoperative follow-up involved with these transfers. The importance of a thorough assessment of the patient’s deficits and goals is emphasized, along with proper management of expectations and associated risks. Technical details of tendon harvest, tendon tunneling, pulley formation, and tension-setting are outlined. Helpful tips and tricks are included to streamline the steps and avoid pitfalls. Common modifications to optimize function are also discussed. At the end of this chapter, the reader should be familiar with the key features of low median nerve palsy tendon transfers, the unique advantages and disadvantages of each, and the judicious use of preoperative evaluation and intraoperative decision-making to increase the likelihood of success.
8.1 Description
Low median nerve palsy tendon transfers are directed toward restoring thumb opposition, a critical primate function for both power and precision manipulation.
8.2 Key Principles
8.2.1 General Principles of Tendon Transfers
The following set of “rules” or principles represents an essential guide to performing tendon transfers and optimizing the likelihood of success 1 , 2 :
Supple joints: A tendon transfer will not move a stiff joint. After nerve injury, the joints must be kept supple with the aid of supervised hand therapy and home exercises. If a joint contracture develops, it must be corrected prior to tendon transfer, as the latter requires a period of postoperative immobilization, while contracture release dictates immediate mobilization. 1
Soft tissue equilibrium: The surrounding soft tissues must reach a state of equilibrium: there should be no active open wounds, no inflammation, and all scars should be soft and mature. Generally, the path for tendon transfer is established in the subcutaneous plane. If excessive scar is present, it may have to be excised and replaced with new soft tissue via regional or free tissue transfer. Alternatively, the tendon transfer is re-routed along a different path.
Adequate strength of tendon: The transferred tendon should be strong enough to move the desired joint. Typically, the process of transfer weakens the tendon by one grade. 1
Adequate excursion of tendon: Every attempt should be made at matching the excursion amplitude of the transferred tendon to that of the tendon it replaces. Excursion amplitude represents the linear motion of the muscle-tendon unit as it contracts. In general, extrinsic finger flexors have an excursion amplitude of 70 mm, extrinsic finger extensors of 50mm, and extrinsic wrist flexors and extensors of 30mm. 1 If the donorrecipient tendon excursion cannot be matched, one can supplement the active range of motion by tenodesis effect.
Straight line of pull: The transferred tendon should ideally run in a straight line from its origin to its new insertion. If this is not possible, pulleys should be utilized.
One tendon, one function: Tendon transfers are generally most successful when the transferred tendon performs one function.
Expendable donor: Loss of function associated with donor tendon sacrifice should not be critical to hand function. For example, extensor indicis proprius (EIP) opponensplasty does not sacrifice index finger extension given the presence of a separate extensor digitorum communis (EDC) tendon to the index finger.
Synergy: Tendon transfer by default necessitates a period of re-education for the patient (i.e., in EIP opponensplasty, EIP tendon’s new function is to move the thumb rather than the index finger). This process may be easier if “synergistic” tendons are used. For example, wrist flexion and finger extension work in unison when grabbing and gripping objects, i.e., wrist flexors and finger extensors are said to be synergistic. Therefore, in the setting of a radial nerve palsy, a wrist flexor is transferred to restore finger extension. Similarly, in low median nerve palsy tendon transfers, rehabilitation is easier if the transferred muscle-tendon unit is synergistic with abductor pollicis brevis (APB), as is the case with the EIP transfer.
8.2.2 Considerations Specific to Low Median Nerve Palsy Tendon Transfers
Median nerve injuries are divided into high and low depending on whether the injury is proximal or distal to the forearm muscle innervation. 1 In high median nerve injuries, the injury is proximal to the forearm muscle innervation, whereas in low median nerve injuries, the injury is distal to the innervation. Thus, in the low median nerve palsy, pronator quadratus, pronator teres, flexor carpi radialis (FCR), all four FDS, flexor pollicis longus (FPL), and index/middle finger flexor digitorum profundus (FDP) muscles are usually intact and functional, unless also traumatically injured. The muscles affected by the palsy are the thenar muscles and the radial two lumbricals. The intact ulnar-innervated interossei can compensate for the lumbricals, whereas loss of thenar muscles may significantly impact the ability to oppose the thumb. As such, the main goal of tendon transfers in the setting of a low median nerve palsy is restoring thumb opposition, and these transfers, accordingly, are often referred to as opponensplasties or opposition tendon transfers.
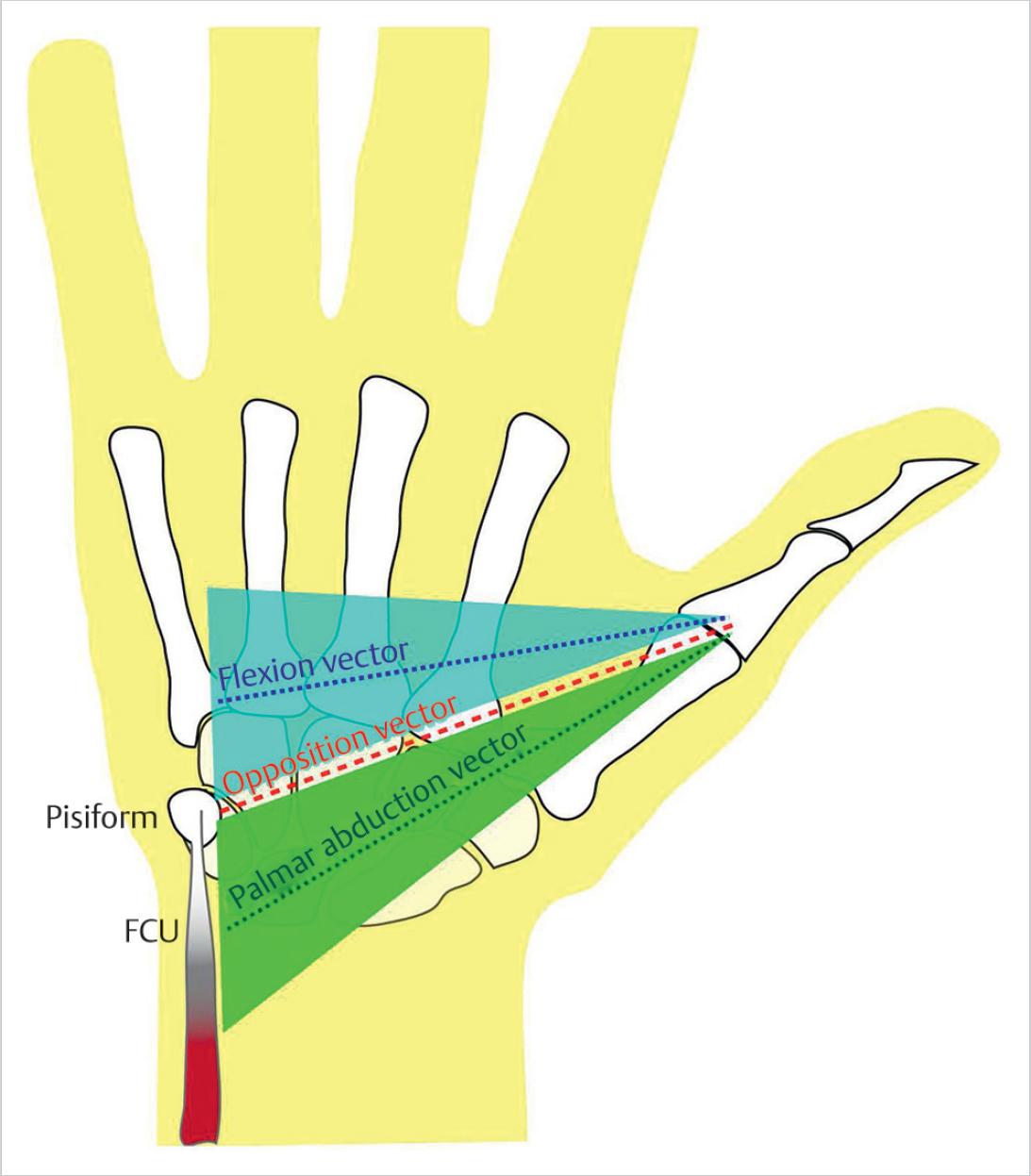
Thumb opposition is a complex movement that consists of palmar abduction, pronation, and flexion. 1 , 2 There are three muscles in the thenar eminence that contribute to opposition: APB, opponens pollicis (OP), and flexor pollicis brevis (FPB). Of these muscles, APB is recognized as the most important for opposition. 3 In cases of an isolated median nerve palsy, the APB insertion on the radial side of the thumb metacarpophalangeal (MCP) joint is a commonly used insertion site for opposition tendon transfers. The ideal line of pull for these transfers starts at the pisiform (► Fig. 8.1). If the line of pull is more distal to the pisiform, a greater degree of thumb flexion is achieved, which can be useful in cases of a combined ulnar and median nerve palsy. 3 If the line of pull is more proximal to the pisiform, a greater degree of thumb abduction is achieved. 3
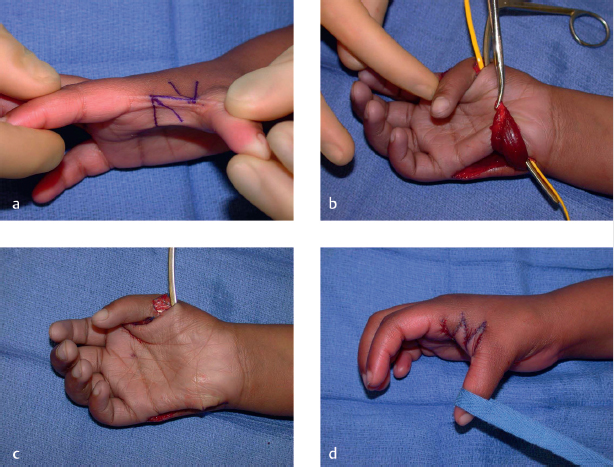
Assessing the soft tissue environment around the thumb is critical for success with opponensplasties. Particular attention should be directed at the status of the dorsal skin and web space. In a long-standing low median nerve palsy, shortening of the dorsal skin and fascia may occur, especially if the patient develops a habit of lateral squeeze pinch. 4 If the contracture is not corrected, the dorsal skin will limit thumb abduction and, especially, pronation. 4 Crank action may develop, which will result in a progressive supination deformity of the thumb with loss of metacarpal abduction and pronation. 4 Thus, before any tendon transfer procedure, the thumb should be assessed for its full ability to oppose passively without limitation. If restrained, passive stretching and splinting will be needed. 4 In more severe cases, a sliding webplasty, Z-plasty, or even free tissue transfer is considered (► Fig. 8.2). 4
8.3 Expectations
Setting reasonable expectations for patients is of paramount importance. Patients should have a good understanding of the reason for surgery and the severity of their injury, specifically the irrecoverable nature of nerve damage that often leads to the need for tendon transfers. A well-executed tendon transfer will at best approximate the original degree of function, not restore it completely. Even if good range of motion and strength are achieved, the act and coordination of a particular movement is never the same as in the premorbid state. The tendons are taken out of their natural context and re-routed to perform a different task, which requires a period of re-education and retraining. Hand therapy, with persistent repetitions, is critical to achieving success. The patient’s willingness and ability to engage in the strenuous rehabilitation process should thus be confirmed prior to surgery. 2
Specific risks associated with each opponensplasty should be discussed. After an FDS transfer, for example, a patient may develop a weakened grip due to ring finger donor tendon sacrifice. 2 , 3 After an EIP tendon transfer, a patient may not be able to independently extend the index finger developing a small degree of extensor lag. 2 , 3 The patient should understand the potential need for an additional tendon graft if the transferred tendon is too short.
8.4 Indications
Historically, polio was one of the earliest and most common indications for tendon transfers, including opponensplasties as a result of thenar muscle paralysis. 1 , 2 , 3 Today, the most common indication for a tendon transfer is a nerve injury that has little-to-no chance of recovery. 1 This can happen in the context of a traumatic injury (i.e., median nerve laceration, failed median nerve reconstruction/recovery) or a compressive neuropathy (i.e., severe carpal tunnel syndrome). 1 , 2 , 3 By default, high median nerve palsies include low median nerve deficits; therefore, pronator syndrome, cervical radiculopathy, or brachial plexopathy may lead to thenar atrophy and the need for restoration of thumb opposition. Congenital absence of thenar muscles is also possible. 1 , 2 , 3 Finally, low median nerve palsy can occur in the context of specific neurologic maladies such as hereditary spastic paraplegia, cerebral palsy, Charcot-Marie-Tooth disease, or spinal cord injury. 1 , 2 , 3 Although currently not as pertinent, leprosy affects peripheral nerves and may also necessitate tendon transfers. 1
A thorough assessment of a patient’s functional impairment is essential prior to committing to surgery. If the low median nerve palsy is limited to the nondominant hand, a patient may compensate fairly well without an opponensplasty, depending on the required daily activities and demand level. 2 If there is associated loss of sensation, the hand surgeon must make sure that the loss of opposition is not due to sensory deficit. 2 Even if a true lack of motor function exists, a well-executed tendon transfer will not reach maximal potential if the patient cannot sense the moving parts. Sensory nerve transfers may have to be considered. 5 , 6 Finally, not all patients with a low median nerve palsy have significant loss of opposition. Jensen et al noted that only 14% of patients with a median nerve injury required an opponensplasty. 7 Similarly, Foucher et al found that only 6.6% of patients with an operative carpal tunnel syndrome had a severe enough deficit to require treatment for thumb opposition weakness. 8 This may be related to cross-innervation from the ulnar nerve and the resulting compensation by the FPB muscle. The superficial head of FPB, in fact, receives dual innervation by the median and ulnar nerves in 30% of cases, whereas the deep head receives dual innervation in 79% of cases. 9 , 10 Additional anatomic means of compensation exist, through volar slips of abductor pollicis longus (APL) (the so-called digastric muscle of Wood 11 , 12 , 13 , 14 ), recruitment of APL with increasing effort, 15 or action of other radial-innervated muscles such as extensor pollicis brevis. 15 , 16 A recent appraisal of clinical deficits following high median nerve injuries showed that patients still averaged a fairly high 7.5 out of 10 score on the Kapandji opposition scale. 17
8.5 Contraindications
A tendon transfer will not work in the setting of excessive scar, joint contracture, active wound, or inflammation. The procedure is also contraindicated in a patient who refuses to participate in the required hand therapy following surgery, including both the supervised component with a dedicated therapist and the obligatory home exercises. As discussed above, every effort should be made to truly assess the patient’s deficit, as not every case of median nerve palsy has a significant enough opposition defect to require a tendon transfer; the clinical experience of many, in fact, argues otherwise. 7 , 8 , 17 , 18 Particular caution should be taken in unilateral nondominant hand cases or cases that involve a sensory deficit where the disability may be due to loss of sensation rather than true motor loss of opposition. 2
8.6 Special Considerations
Unique considerations exist for each type of opponensplasty. The EIP tendon transfer, for example, is an attractive option in a high median nerve palsy or traumatic injuries that simultaneously affect the extrinsic flexor tendons, precluding the use of FDS. 2 , 3 Furthermore, there is less risk of grip strength loss compared to an FDS transfer. No separate pulley creation is required; the distal ulna itself plays the role of the pulley, which is fairly stable, limiting the propensity of the tendon transfer to migrate. 2 One potential drawback of the transfer is that patients may develop an extensor lag or lose the ability to independently extend the index finger. 3 The former risk presumably can be mitigated by not harvesting any part of the extensor hood with the EIP tendon. 19 Rarely, a tendon autograft may be needed if the harvested EIP tendon has insufficient length. EIP also has a shorter muscle-fiber length compared to APB and the ring FDS, which may limit the resulting degree of thumb motion. 2
In the FDS transfer, the ring finger FDS is typically used. This, however, carries a risk of grip strength weakness, which has led some to favor the middle finger FDS. 2 The middle finger FDS is also considered in combined median-ulnar nerve injuries, as the ring FDP is ulnar-innervated and harvesting the ring FDS may deprive the ring finger of all its extrinsic flexor function. 3 FDS transfer is contraindicated in high median nerve palsies, given the muscle’s median nerve innervation.
PL transfer is very convenient when performing a simultaneous carpal tunnel release. 2 , 3 , 20 Additionally, there is no functional morbidity associated with this tendon sacrifice. In about 15 to 20% of individuals, however, PL is congenitally absent. 3 Special caution should be exercised in traumatic wrist or forearm injuries where PL may have been transected or the surrounding soft tissue and overlying skin have become too scarred for successful harvest and re-routing of the tendon. 2 It is reasonable to ask whether a Camitz transfer is truly indicated at the time of carpal tunnel release, as some thenar muscle function may recover after median nerve decompression. However, the amount of recovery is unpredictable and even if successful, the recovery may take significant time. 2 Given the convenience of the transfer and its low functional morbidity, our preference is to perform the transfer at the same time as the carpal tunnel release rather than wait for recovery if there is a true opposition deficit.
ADM transfer is a very practical transfer. It limits the operation to the palm, does not involve significant re-routing or pulley formation, and replaces an absent or atrophied thenar APB with a similarly sized hypothenar muscle. 2 , 3 As such, it is particularly useful in forearm trauma cases, where harvest of palmaris or FDS may not be possible and EIP may not be successfully tunneled through the forearm scar. If APB is congenitally absent or severely atrophied, ADM can add bulk to the thenar eminence, thus restoring not only function but form. 2 , 3 ADM also contracts and shortens throughout its length, not relying on tendon gliding as much as the other transfers. Because it is an intrinsic muscle and does not cross the wrist joint, it also avoids issues associated with tenodesis. 21
Related posts:
 7 Radial Nerve Palsy Tendon Transfers
7 Radial Nerve Palsy Tendon Transfers
 6 Flexor Tendon Reconstruction (Zone 2)
6 Flexor Tendon Reconstruction (Zone 2)
 10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
 9 Tendon Transfers for Low Ulnar Nerve Palsy
9 Tendon Transfers for Low Ulnar Nerve Palsy
 11 Extensor Indicis Proprius to Extensor Digitorum Communis Tendon Transfer
11 Extensor Indicis Proprius to Extensor Digitorum Communis Tendon Transfer
 12 Superficialis Transfer for Rupture of the Flexor Pollicis Longus Tendon
12 Superficialis Transfer for Rupture of the Flexor Pollicis Longus Tendon
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


