7 Radial Nerve Palsy Tendon Transfers
Abstract
Various tendon transfer options exist to restore hand and wrist function following radial nerve palsy. Donor selection principles are critical to successful transfers. Tendon transfer principles are applied including an expendable donor, synergistic function, similar excursion and power, straight line of pull, and one transfer for one function. Surgical indications, tips, recommended techniques, and salvage procedures are reviewed in detail.
7.1 Description
Various tendon transfer options are available for radial nerve palsy in the setting of proper functioning median and ulnar nerves (► Table 7.1). 1 The aim is to restore wrist, metacarpophalangeal (MCP) joint, and thumb extension. Interphalangeal (IP) joint extension is typically preserved with the unaffected intrinsic muscles.
7.2 Key Principles
The level of radial nerve injury dictates the interventions necessary to restore functional motion. In low radial nerve or posterior interosseous nerve injury, where extensor carpi radialis longus (ECRL) wrist extension is spared, reconstruction should focus on restoring finger and thumb extension. In pre-radial bifurcation nerve injury, wrist extension should also be restored.
In order for a muscle group to be considered transferable, it must follow these basic principles 2 :
The donor muscle must be expendable and loss of its primary function should not significantly compromise the patient’s residual functional motion and strength.
The donor unit must have at least full active motion against resistance, since transfer causes an expected loss of at least one grade of strength. Ideally, the force generation of the donor should be equal to or greater than the recipient it is replacing.
Donor transfers must have sufficient amplitude of tendon excursion similar to the recipient and be in a straight vector, ideally crossing a single joint.
One tendon transfer should be considered for one specific function.
Knowledge of available muscle units is important as well. Always assess and prioritize which functions need to be restored and which muscle-tendon units are viable donors. In partial radial nerve palsies, some extensor groups are spared and attention should be directed to restoring the remaining functional deficits. Alternatively, if the patient is missing a muscle group from a concurrent injury, prior transfer, or congenital absence (i.e., palmaris longus [PL]), then alternative donors should be investigated. Synergistic muscles are preferred due to ease of rehabilitation. For example, wrist flexors and digit MCP extensors are usually contracting simultaneously, so postoperative occupational therapy is more intuitive than a finger flexor to finger extensor transfer.
7.3 Expectations
Injuries proximal to the elbow cause high radial nerve palsies, and tendon transfers are used to restore the resulting motor deficits in wrist extension, lesser digit MCP extension, and thumb extension. Injuries distal to the elbow cause low radial nerve palsies, often with preserved wrist extension from the ECRL. In low radial nerve injuries, tendon transfers restore lesser digit extension at the MCP joints and thumb extension.
The pronator teres (PT) is typically transferred to the extensor carpi radialis brevis (ECRB) as it inserts centrally on the hand at the base of the third metacarpal, which can create more neutral extension than the ECRL insertion on the second metacarpal. Flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU) are common donors for lesser digit extension. PL or the ring finger flexor digitorum superficialis (FDS) can be transferred to the extensor pollicis longus (EPL). FCR transfer to the first compartment extensors is less common. 2
7.4 Indications
Tendon transfers should be considered when there is loss of wrist extension, finger extension at the MCP joint, and thumb extension secondary to radial nerve injury with a poor prognosis for functional recovery due to known anatomic features, electrophysiologic, or minimal clinical improvement by 6 months after the injury.
7.5 Contraindications
Absolute:
Lack of appropriate donors tendon/muscle (which may be from concomitant median and ulnar nerve injury)
Muscle-tendon units with less than grade 4 strength
Severe joint contractures and ankylosis
Active infection
Inability to cooperate with postoperative restrictions and rehabilitation
Relative:
Donor muscle-tendon units with less than grade 5 strength
Moderate joint contractures
Soft tissue bed inflammation and sclerosis
7.6 Special Considerations
EMG and nerve conduction studies may be helpful 3 months following the injury in order to confirm radial nerve deficits or failure of spontaneous recovery. If clinical or electrophysiologic evidence of recovery is not present at 4 to 6 months, the prognosis for robust nerve recovery is poor. Preoperative passive range of motion should be assessed to ensure supple joints are present to accept tendon transfers. Patients with progressive neurological disorders affecting peripheral nervous system may be a poor candidate for tendon transfer due to possible neighboring involvement of nerves. It is also necessary to determine patient’s functional needs to ensure appropriate affected motions are restored.
7.7 Special Instructions, Positioning, and Anesthesia
A regional nerve block may be helpful in reducing amount of general anesthesia
Supine position with operative extremity extended on a hand table
Careful preoperative observation and assessment of particular donor muscle strength
Determine particular muscle units available for transfer
If multiple incisions are necessary, leave ample distance between them for primary closure
If soft tissue deficits are present and primary closure is unobtainable, consider rotational or free flap coverage at the time of tendon transfer
Preoperative occupational therapy may be used to keep the wrist and hand joints supple
7.8 Tips, Pearls, and Lessons Learned
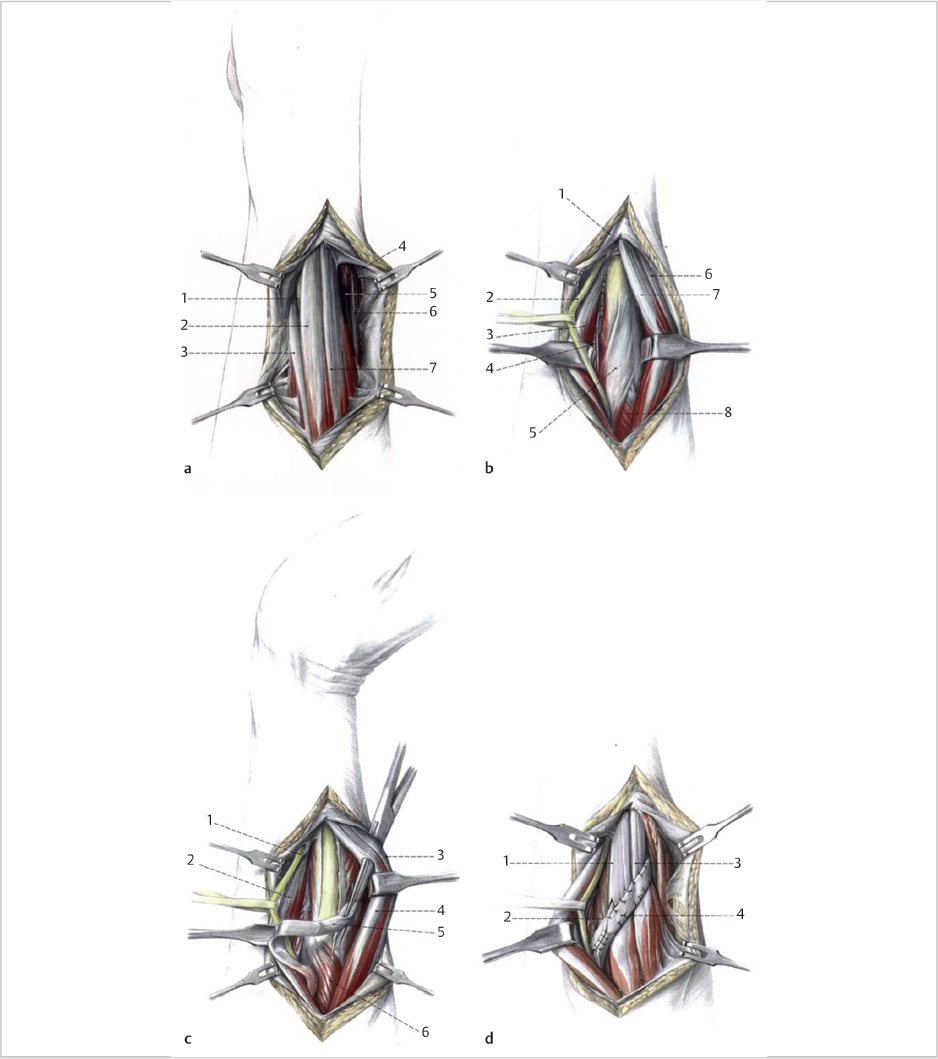
7.8.1 PT Donor
Harvest the tendon with a 3-cm extension of periosteum from the radial shaft to increase the effective tendon length for weaving. Routing the PT subcutaneously and superficial to the brachioradialis (BR) and ECRL can minimize adhesions (► Fig. 7.1).
Related posts:
 6 Flexor Tendon Reconstruction (Zone 2)
6 Flexor Tendon Reconstruction (Zone 2)
 8 Low Median Nerve Palsy Tendon Transfers
8 Low Median Nerve Palsy Tendon Transfers
 10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
 9 Tendon Transfers for Low Ulnar Nerve Palsy
9 Tendon Transfers for Low Ulnar Nerve Palsy
 11 Extensor Indicis Proprius to Extensor Digitorum Communis Tendon Transfer
11 Extensor Indicis Proprius to Extensor Digitorum Communis Tendon Transfer
 12 Superficialis Transfer for Rupture of the Flexor Pollicis Longus Tendon
12 Superficialis Transfer for Rupture of the Flexor Pollicis Longus Tendon
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


