Abstract
SAFELipo differs from traditional liposuction and was developed to overcome its shortcomings. Whereas traditional liposuction is strictly a reductive procedure, SAFELipo is a comprehensive body contouring technique for fat, skin, and the fasciocutaneous network. SAFELipo allows the surgeon to expand the resistance differential between tissue planes, whether the goal is to remove more fat, release fibrous scar, redistribute residual fat, or add more fat to the area using expansion vibration lipofilling (EVL). This technique allows for dramatic and thorough liposuction without increasing the risk of contour deformities or damage to the skin and blood supply. It is more than a reductive or additive procedure because it removes, redistributes, blends, and adds fat as needed. It releases and equalizes disparities in skin distribution, simultaneously providing for areas of skin retraction much wider than traditional liposuction treatment areas. SAFELipo also treats deep and superficial tissues without disrupting vascular and stromal networks.
74 SAFE Liposuction
Key Points
Heat generated by radiofrequency, ultrasound, and laser liposuction causes ischemia, cell death, and inflammation—all detriments to creating a smooth, natural result.
The three-step process of SAFELipo (separation, aspiration, and fat equalization) allows greater control, precision, and safety in fat manipulation.
SAFELipo separation widens the resistance differential which gives the surgeon greater control and precision in manipulating the adipose tissue.
Fat equalization emulsifies some of the remaining fat, eliminates thicker and thinner areas of fat, and leaves this liquified fat as a smooth layer of local fat grafts to prevent adherence and fill in any imperfections.
SAFELipo and expansion vibration lipofilling (EVL) are ideal for treating contour deformities, with the majority of time spent in the separation, equalization, and expansion phases for correction of irregularities.
74.1 Preoperative Steps
Poor skin quality (striae, atrophic type cellulite/dimpling, laxity) can compromise the result and needs to be noted and discussed with the patient.
Delineate and discuss the fat distribution pattern: intra-abdominal versus extra-abdominal fat and apple versus pear shape.
Evaluate the muscular framework and define the patients’ goals to discern their expectations (lean/thin versus big/broad).
Carefully examine for any hernias—failure to recognize a fascial defect can lead to a catastrophic visceral injury.
Skeletal asymmetries (scoliosis, leg-length discrepancies, pelvic tilt, and chest wall deformities) need to be documented and discussed with the patient.
Patients with a body mass index (BMI) of over 30 typically have a large amount of visceral fat, and it is more difficult to create a rewarding postoperative result. They also have a higher perioperative complication rate.
Zones of adherence or tethering within the treatment area do not need to be avoided, but rather they need to be clearly marked out preoperatively, as these areas need additional time spent in the separation and equalization phases.
Carefully plan intraoperative patient positioning, and discuss with the surgical team. For circumferential trunk SAFELipo only, we prefer a 360-degree prep and use a supine–lateral–lateral sequence. For SAFELipo with safe subcutaneous buttock augmentation (SSBA), we use all four positions adding prone to the supine–lateral–lateral sequence.
74.2 Operative Steps
See Video 74.1.
74.2.1 Positioning
Carefully plan intraoperative patient positioning, and discuss with the surgical team.
We prefer a single whole-body prep so that the patient can be moved frequently into any position intraoperatively rather than struggling from fixed positions.
For circumferential trunk SAFELipo, we use a supine–lateral–lateral sequence.
Although the epigastric–thoracic transition area can be treated from the supine position, it is safer and easier from the lateral decubitus position because the adipose tissue falls away from the fascia.
Treating targeted areas from multiple hidden access sites and patient positions increases cross-hatching and reduces the likelihood of contour irregularities.
74.2.2 Infiltration
Good infiltration with simultaneous separation and tumescence (SST) provides for wide dispersion and immediate vasoconstriction with initial fat separation, ultimately reducing vascular injury and improving surgeon awareness and control of cannula position by eliminating flexibility misguidance and increasing working space.
For primary liposuction cases, we recommend an infusion-to-aspiration ratio of 1:1 or 1.5:1.
In a repeat liposuction procedure (or in patients with highly fibrotic-tethered tissues), additional volume expansion of the target zone is even more vital to being able to precisely traverse the tissue planes, and a tumescent approach with a ratio of 2:1 or even 3:1 utilizing SST is frequently required.
Assuming patients have no cardiac, pulmonary, or renal medical history, it is not uncommon to use 6 to 10 L of infiltration when planning to aspirate 3 to 7 L of fat.
74.2.3 Separation
Separation (including infiltration with SST) accounts for 40% of the total procedural time in primary SAFELipo (Fig. 74.1 and Fig. 74.2).
Separation is the process of widening the resistance differential between the target fat and surrounding structures using rapid oscillations of a 4 to 5 mm angled exploded-tip cannula through the adipose tissue to mechanically emulsify the solid fat architecture into a more liquid environment.
We recommend power-assisted liposuction (PAL) for separation to maximize the oscillations and efficacy of the wings on the exploded-tip cannulas and to minimize effort during liposuction.
In repeat liposuction cases, the separation step is more critical because the adipose layer can be scarred; scarring narrows the resistance differential between target fat and other, unintended structures, and makes it more difficult for the surgeon to precisely treat this layer.
The endpoint of the separation step is the loss of resistance with cannula passage, indicating a very wide resistance differential and adequately emulsified fat.
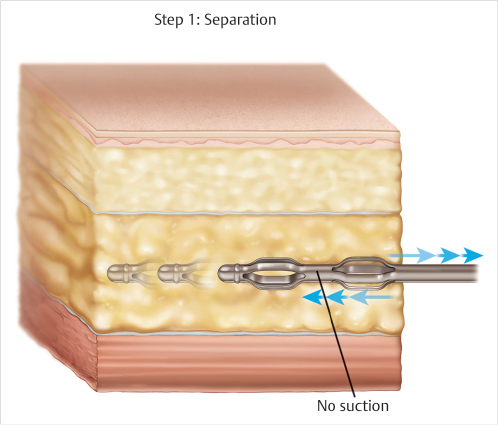
Fig. 74.1 Cross section of adipose tissue, before separation.
(Reproduced with permission from Steinbrech DS. Male Aesthetic Plastic Surgery. Thieme; 2020.)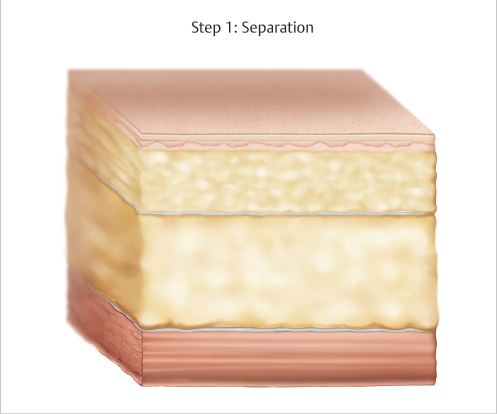
Fig. 74.2 Cross section of adipose tissue, after separation.
(Reproduced with permission from Steinbrech DS. Male Aesthetic Plastic Surgery. Thieme; 2020.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


