60. Abdominoplasty
Anatomy
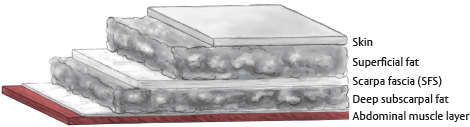
The abdominal wall is composed of seven layers.
Skin
Subcutaneous fat
Scarpa fascia (the superficial fascial system of the abdomen)
Subscarpal fat
Anterior rectus sheath
Muscle
Posterior rectus sheath
Skin
The skin of the abdominal wall receives a rich vascular supply from multiple muscle and fascial perforating vessels.
The skin of the abdominal wall can vary in quality depending on a person’s genetics, age, previous pregnancies, and history of weight gain and loss.
The skin of the abdominal wall may feature multiple striae, which are evidence of attenuated or absent dermis.
Fat
The abdominal wall has two layers of fat, superficial and deep, separated by Scarpa fascia (Fig. 60-1).
The superficial layer of fat is thicker, more dense, more durable, and has a heartier blood supply.
The deeper layer of fat is less dense and receives most of its blood from the subdermal plexus and underlying myocutaneous perforators.
Senior Author Tip:
Because the blood supply to the deeper fat is distinct from the blood supply to the skin, it can be more easily excised when thinning the abdominal wall flap in an abdominoplasty. By contrast, thinning the superficial layer of fat may lead to vascular compromise of the overlying skin
There are four paired muscle groups of the abdominal wall.
Rectus abdominis
External oblique
Internal oblique
Transversus abdominis
The aponeurotic portions of the transversus muscle and the two oblique muscles envelop the rectus abdominis muscles, forming the anterior and posterior rectus sheaths and meeting in the midline to form the linea alba.
The arcuate line represents a transition point.
Above the arcuate line, there are distinct anterior and posterior rectus sheaths.
Below the arcuate line, contributions from the internal oblique and transversus abdominus join contributions from the external and internal obliques to form a single anterior rectus sheath with no posterior rectus sheath.
The arcuate line is roughly halfway between the umbilicus and symphysis pubis.
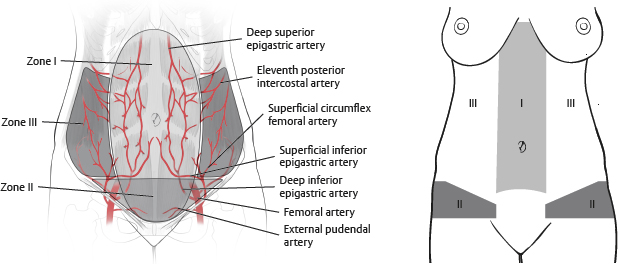
Vascularity of the Abdominal Wall
Huger 1 divided the vascular supply to the abdominal wall into three zones (Fig. 60-2).
Zone I
Between the lateral borders of the rectus sheath from the costal margin to a horizontal line drawn between the two anterior superior iliac spines (ASIS)
Supplied primarily by superficial branches of the superior and inferior epigastric systems
Zone II
Below the horizontal line between the two ASISs to the pubic and inguinal creases
Supplied by the superficial branches of the circumflex iliac and external pudendal vessels
Zone III
Superior to zone II and lateral to zone I
Supplied by intercostals, subcostals, and lumbar vessels
Sensation to the abdomen is from intercostal nerves T7-12.
Nerves and the Abdominal Wall
Lateral Cutaneous Branches
Perforate the intercostal muscles at the midaxillary line
Travel within the subcutaneous plane
Anterior Cutaneous Branches
Travel between the transversus abdominus and internal oblique muscles to penetrate the posterior rectus sheath just lateral to the rectus
Eventually enter the rectus muscles and then pass to the overlying fascia and skin
Lateral Femoral Cutaneous Nerve
Innervates the skin in the lateral aspect of the thigh
Emerges close to the ASIS
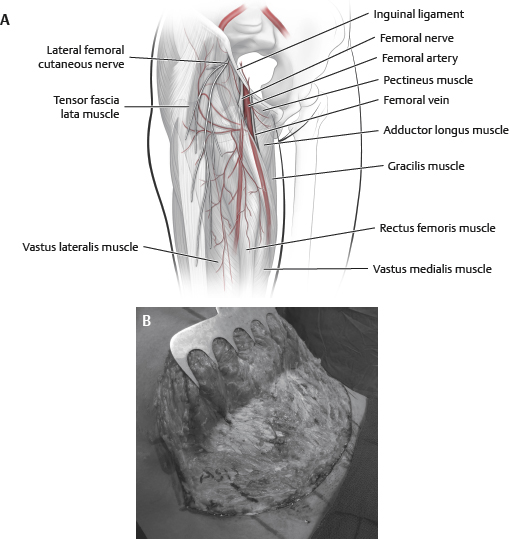
Tip:
To prevent injury, a layer of fat should be left over the ASIS
The umbilicus is located on or near the midline at the level of the iliac crest.
The umbilicus is located exactly in the midline of the body in only 1.7% of patients. 2
An aesthetically pleasing umbilicus has the following characteristics 3 :
Superior hooding
Inferior retraction
Round or ellipsoid shape
Shallow
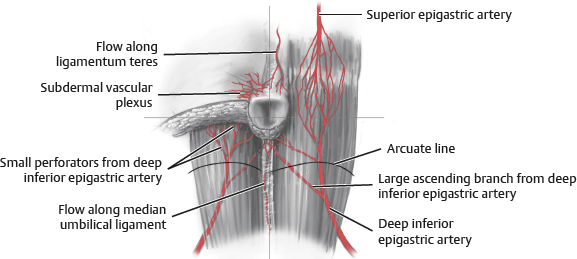
Blood supply to the umbilicus (Fig. 60-4) is from:
Subdermal plexus
Right and left deep inferior epigastric artery (DIEA)
Ligamentum teres
Median umbilical ligament
Aesthetic Aspects of Abdominoplasty
Incision should be low and symmetrical
Umbilicus
Inverted scar
Superior hooding
Circular or ellipsoid
Scaphoid abdominal wall
Smooth transition at the incision
Aesthetic appearance of mons pubis
Indications and Contraindications
Due to the number of variations of the abdominoplasty procedure, it is key to select the appropriate technique for each patient to minimize morbidity and deliver the intended result (Table 60-1). 5 Selection of appropriate technique is based on the patient’s expectations and physical examination.
Contraindications
Absolute
Significant health risks, unrealistic surgical goals, and body dysmorphic disorder are primary contraindications for an abdominoplasty.
Relative
Right, left, or bilateral upper abdominal scars
Severe comorbid conditions (e.g., heart disease, diabetes, morbid obesity [BMI >40], cigarette smoking)
Plans for future pregnancy
A history of thromboembolic disease
Subcostal scars are particularly concerning, and many of these patients are not optimal candidates for a traditional abdominoplasty.
These scars represent an interruption in the blood supply upon which the abdominoplasty flap will rely postoperatively.
Patients with a disposition to keloid formation or hypertrophic scars have to be accepting of the poor scarring associated with these conditions.
Gross deformity in adjoining areas may lead to disfiguring results and poor patient satisfaction.
Most massive-weight-loss patients are not candidates for abdominoplasty alone and will require circumferential procedures.
Increased intraabdominal pressures can lead to serious problems postoperatively, possibly resulting in abdominal compartment syndrome.
In cases of elevated intraabdominal pressure, the abdominal wall elevates above a line between the costal margin and iliac crest in the supine position.
Abdominoplasty procedures with or without rectus plication have to be performed cautiously in the nonscaphoid abdomen.
Preoperative Evaluation
Assessment must include a detailed medical history with specific focus on:
Prior cesarean section or other abdominal surgeries
Pregnancy history
Weight fluctuations and stability
Prior liposuction in the abdominal area
Thromboembolic risk
Smoking status
Hormone use
History of postoperative nausea and vomiting (PONV)
Tip:
Abdominoplasty is an enormous stressor in terms of blood supply to the abdominal wall. To minimize complications, avoid operating on active smokers. If a patient has a history of smoking, insist that the patient quit smoking prior to the procedure. A thorough discussion of the increased risk of complications associated with smoking must occur. In certain cases, a urine nicotine test may be warranted preoperatively and postoperatively should complications occur
Other patient factors to consider include:
Weight fluctuations and constancy
Exercise routine
Gastrointestinal history including irritable bowel syndrome or constipation
Cardiac and pulmonary history (including obstructive sleep apnea)
Desire for future pregnancy (patients should be encouraged to wait)
Physical examination must explore the existence and localization of vertical and horizontal abdominal tissue excess and its relation to the underlying abdominal wall; deformity present in adjoining areas must be noted as they affect the final result.
Tip:
If the patient is examined only in the standing or supine positions, one may be fooled into thinking there is little to no excess skin. The patient must be examined while standing, sitting, and supine
Musculofascial laxity must be thoroughly assessed (Fig. 60-5).
A diver’s test can be performed with the patient first standing and flexing at the waist; worsening of lower abdominal fullness indicates significant laxity (see Fig. 60-5).
The pinch test can also be performed. If tensing the abdominal wall significantly decreases the amount of fullness, significant laxity is present.
Midline rectus diastasis must be assessed by palpation of a tensed abdominal wall in the supine position.
Tip:
Nearly all patients who have been pregnant have some degree of musculofascial laxity of the abdominal wall in addition to excess skin

Preoperative identification of any existing ventral or umbilical hernia is imperative. Examination should include evaluation for incisional, epigastric, periumbilical, and inguinal hernias—especially in patients with prior abdominal surgeries and massive weight loss.
Tip:
The importance of a thorough hernia examination cannot be overstated. Preoperative knowledge of hernias can help the surgeon avoid bowel injury during dissection. Depending on the site of the hernia and the comfort level of the plastic surgeon, preoperative knowledge of a hernia may allow repair to be coordinated with a general surgeon. In cases of uncertainty, a computed tomography (CT) scan is indicated
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


