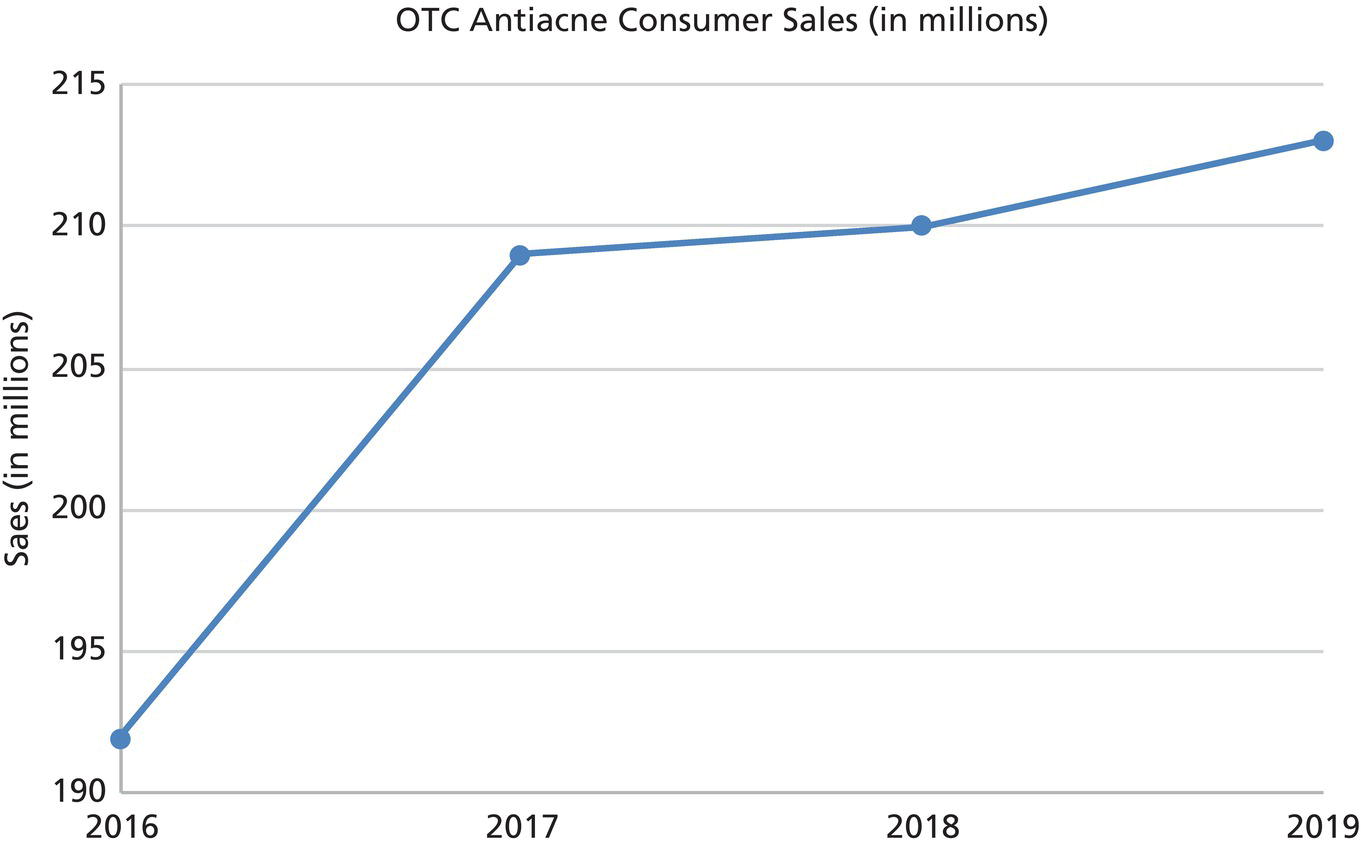
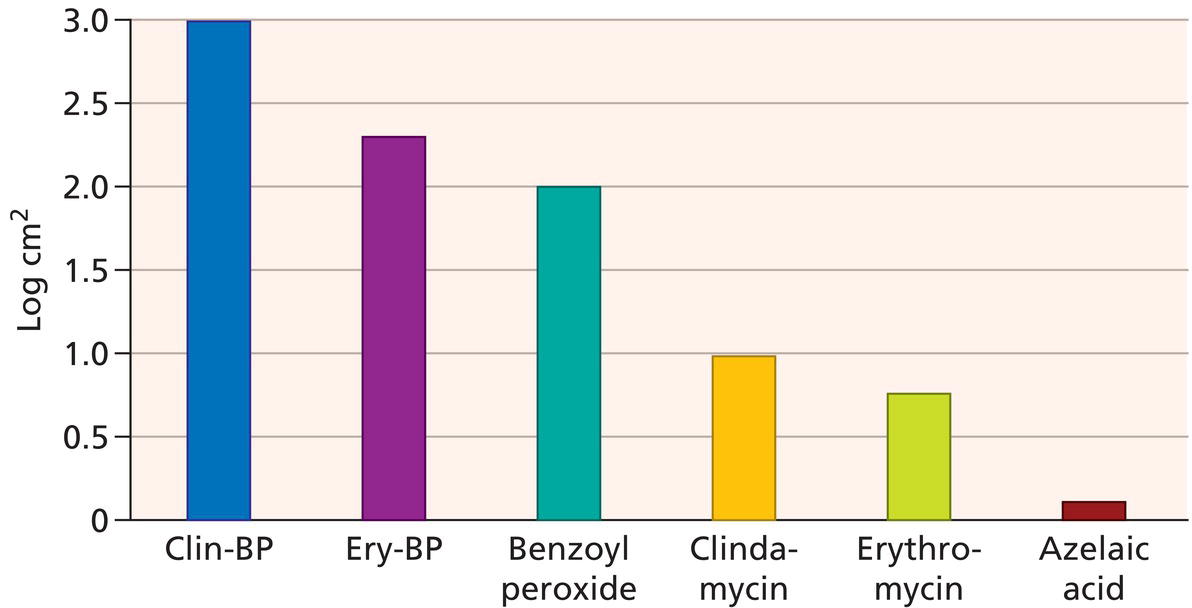
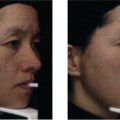
Kirsten Swenson1, Emmy M. Graber1,2, and Diane Thiboutot3 1 The Dermatology Institute of Boston, PC, Boston, MA, USA 2 Affiliate Clinical Instructor Northeastern University, Boston, MA, USA 3 Pennsylvania State University College of Medicine, Hershey, PA, USA Although acne is one of the most common conditions that a general dermatologist treats [1], most people with acne will first try to self‐treat before seeking the assistance of a healthcare professional. A survey carried out in 2000 demonstrated that 75% of acne sufferers waited about 1 year prior to seeking the help of a healthcare professional [2]. Another study estimated that one‐third of those battling acne will ever consult a physician regarding their condition [3]. Without the assistance of a physician, patients will often turn to the drugstore shelves to treat their acne. A plethora of over‐the‐counter (OTC) modalities exists for treating acne. These modalities include topical cleansers, creams, lotions, gels, and masks as well as mechanical treatments, essential oils, and oral vitamins. The non‐prescription acne market is one of the fastest growing segments of the dermatologic industry. This OTC market worldwide is estimated to be 2–4 times the size of the prescription market. In 2019, it was estimated that consumers spent approximately $213 million on OTC antiacne products. The market has steadily increased since 2001, where it was estimated that consumers spent approximately $100 million on OTC antiacne products (Figure 57.1) [4, 5]. The Food and Drug Administration (FDA) is the regulatory agency that presides over the marketing of non‐prescription acne products. In the Final Acne Monograph, the FDA states that any product labeled as an “acne drug product” is defined as: “A drug product used to reduce the number of acne blemishes, acne pimples, blackheads and whiteheads.” The FDA defines OTC products that fit this description to include: salicylic acid (SA), sulfur, sulfur combined with resorcinol, and benzoyl peroxide [6]. Although products cannot be sold bearing an antiacne label unless they contain one of the above‐approved ingredients, many other products are marketed toward the acne‐prone consumer claiming to “heal,” “purify,” or “cleanse,” the skin and pores. In this chapter, we address OTC products that are marketed for the treatment of acne, not just those products that the FDA defines as an “acne drug product.” There are a multitude of OTC products with labelling that implies an acne efficacy. Some of these washes and leave‐on products contain benzoyl peroxide, SA, alpha‐hydroxy acids, polyhydroxy acids, lipohydroxy acids (LHAs), retinol, azelaic acid, or sulfur. Mechanical treatments exist as well and come in the form of cleansing brushes, adhesive pads, heating devices, light devices, and scrubs. Some patients may turn to homeopathic remedies such as tea tree oil or chamomile. Oral vitamins, such as vitamin A, zinc, or nicotinamide are also tried as an OTC acne fix. Studies show that over half of those with acne believe that their condition is caused by poor hygiene and dirt on the skin [7]. This belief often leads patients to alter both how they wash their face and their face washing frequency. While washing the face twice daily is more optimal than washing once or four times daily, the quantity of cleansings probably does not matter as much as the substance that is used to wash the face [8]. A multitude of cleansers exist and can be categorized as either soaps or syndets. Traditional soaps are made of fats and an alkali and have a basic pH of 9–10. This pH, which is higher than the skin’s pH, disrupts the intercellular lipids that hold the stratum corneum together. The disintegration of the intercellular “cement” causes skin irritation. Syndets are made of synthetic detergents and have a pH of 5.5–7, similar to the skin’s natural pH. Because syndets only contain less than 10% soap, they are much less damaging to the stratum corneum [9]. The benefit of syndet cleansers specifically for acne patients has been demonstrated in studies. In one study, 25 patients undergoing acne treatment were randomized to cleanse with either a soap or a syndet. After 4 weeks, those using the syndet cleanser reported having significantly less acne and less oil. Both patients and dermatologists reported less irritation in those using the syndet cleanser [10]. Although not all‐inclusive, some brands of syndet cleansers include Cetaphil, Aveeno, Purpose, Basis, Oil of Olay, and Dove. There are additional cleansers that are marketed specifically for acne use that contain an active antiacne ingredient (e.g. benzoyl peroxide or SA). More recently, micellar cleansers have been growing in popularity for individuals with sensitive skin. These cleansers, composed of surfactants, have been shown to be less irritating on skin than some of the other cleansers on the market, as well as marked improvement in maintaining a healthy skin barrier [11]. Micellar water cleansers are a combination of water and mild surfactants, which produce a dilute cleansing solution [12]. A micelle is an amphipathic molecular structure in which the hydrophobic end interacts to the oil on the skin allowing the hydrophilic end to dissolve the soil in water, cleansing the face. The micellar water cleansers work by emulsification and work efficiently as a facial cosmetic remover [12]. Benzoyl peroxide is commonly found in OTC antiacne washes, creams, and lotions. In fact, 23% of people aged 13–27 have used an OTC benzoyl peroxide product [13]. Benzoyl peroxide was first utilized in 1917 to bleach flour. In the 1960s, benzoyl peroxide began to have medical applications for treating leg and decubitus ulcers. Several years later, in 1979, it was first used for treating acne. Benzoyl peroxide has antibacterial, anti‐inflammatory, and comedolytic properties, which makes it effective in acne treatment. When benzoyl peroxide is absorbed in the skin, it is converted to benzoic acid. Five percent of the benzoic acid is absorbed and excreted in the renal system, and the remainder is metabolized by cysteine in the skin where bacterial proteins are oxidized [14]. It has antimicrobial properties against Cutibacterium acnes (formerly known as Propionibacterium acnes) and Staphylococcal aureus. One study demonstrated an almost 2‐log10 decrease in C. acnes concentration just after 2 days of 5% benzoyl peroxide use [15]. Another study confirmed this fast‐acting effect, showing that C. acnes counts reduced by a mean of 2‐log10 after applying 10% benzoyl peroxide cream for 3 days. After 7 days, there was no further decline in C. acnes levels [16]. Benzoyl peroxide has greater antimicrobial properties against C. acnes than any of the topical antibiotics alone. However, unlike the antibiotics, benzoyl peroxide will not induce bacterial resistance. Using a topical antibiotic with the addition of benzoyl peroxide will increase the bactericidal effect of the antibiotic [17]. Furthermore, it will also prevent the development of C. acnes resistance when used in combination with a topical or oral antibiotic [18]. Figure 57.1 Trends in consumer sales in OTC antiacne medications from 2016 to 2019 according to the Consumer Product Healthcare Association. Benzoyl peroxide also acts as an anti‐inflammatory agent by reducing oxygen free radicals and also by lessening C. acnes density. The reduction of C. acnes has a profound anti‐inflammatory effect since C. acnes induces monocytes to produce tumor necrosis factor α (TNF‐α), interleukin‐1β, and interleukin‐8 [19, 20]. The strong anti‐inflammatory and antibacterial effects of benzoyl peroxide can be parlayed into good clinical results, as shown in a large UK study. This study looked at five antimicrobial acne treatments over an 18‐week period. Subjects used either oral oxytetracycline, oral minocycline, benzoyl peroxide, separate administration of either topical erythromycin or benzoyl peroxide, or a combination product containing both topical erythromycin and benzoyl peroxide. The 5% benzoyl peroxide used twice daily had similar efficacy to 100 mg minocycline once daily. This study also carried out a cost‐effectiveness analysis and found that the least expensive treatment (benzoyl peroxide) was 12 times more cost‐effective than minocycline [21]. Besides being an anti‐inflammatory, benzoyl peroxide is also comedolytic. One study utilizing the rabbit ear comedogenicity assay showed a 10% reduction of comedones [22]. Another study compared 5% benzoyl peroxide twice daily with 0.05% tretinoin once daily for 8 weeks. Both treatments were “extremely effective” for all acneiform lesions but significantly reduced both open and closed comedones after only 2 weeks (Figure 57.2) [23]. Benzoyl peroxide is available OTC in 2.5–10% strengths and as either washes or leave‐on products (e.g. cream, lotion, gel). Leave‐on products reduce C. acnes counts more than the washes, although both significantly reduce C. acnes on the skin [17]. There is some indication that gel formulations may be more stable and release benzoyl peroxide more consistently than creams and lotions [24]. Equal reductions of acneiform lesions are seen with benzoyl peroxide strengths of 2.5, 5, and 10%. Increasing the strength of benzoyl peroxide seems only to intensify the irritation [25]. Skin irritation to benzoyl peroxide is one of its greatest barriers to use. Redness, stinging, and dryness may be manifestations of irritation. Many patients describe this as an “allergy” to benzoyl peroxide. However, true allergic contact dermatitis to benzoyl peroxide is estimated at only 1–2.5% of patients with acne [26, 27]. Patients should be warned about irritation that may result and should also be told of the propensity for benzoyl peroxide to bleach fabrics and hair. In addition to being available OTC, benzoyl peroxide is also available as a prescription. These prescription products may contain different formulations that may enhance penetration and decrease irritation, although no head‐to‐head trials exist comparing prescription with OTC benzoyl peroxide. Since mouse studies have shown that benzoyl peroxide can produce DNA strand breaks, there has been some question to its carcinogenic potential. However, two case‐control studies showed no correlation between benzoyl peroxide use and skin cancer. Additionally, 23 carcinogenicity studies in rodents produced negative results [13]. Epidemiologic evaluations have shown no association between benzoyl peroxide and malignant melanoma [28]. Due to this suspected carcinogenicity potential, some countries, such as those in the European Union, have banned the use of OTC benzoyl peroxide products and restrict its use to a controlled substance in prescription topicals only. In 2011, the FDA included benzoyl peroxide as a generally recognized as safe and effective (GRASE) active ingredient in OTC topical acne drug products with labelling modifications [29]. Figure 57.2 Reduction in Propionibacterium acnes with topical therapy. Clin‐BP, clindamycin and benzoyl peroxide; Ery‐BP, erythromycin and benzoyl peroxide. (Source: Leden, 2001 [Semin Cutan Med Surg 20, 139–43]. Reproduced with permission of Elsevier.) The hydroxy acids are another common OTC antiacne ingredient found in washes and leave‐on products. There are two main classes of hydroxy acids that are used for treating acne: alpha‐hydroxy acids and beta‐hydroxy acids (Table 57.1). The alpha‐hydroxy acids are water‐soluble, penetrate the epidermis and even into the dermis at higher concentrations. They act by desquamating the stratum corneum (i.e. exfoliation). Specifically, alpha‐hydroxy acids disrupt corneocyte adhesion in the upper stratum corneum, possible by chelating calcium [30]. This results clinically in a smoother appearance to the skin, and may also give the illusion of reducing pore size [31]. Alpha‐hydroxy acids also promote epidermolysis, disperse basal layer melanin, and when strong enough to penetrate the dermis they may increase collagen synthesis [32]. These effects may make alpha‐hydroxy acids helpful for acne prevention and treatment of postinflammatory hyperpigmentation. The most common OTC alpha‐hydroxy acids are glycolic acid (derived from sugar cane) and lactic acid (from sour milk) and are found in less than 10% concentration. Table 57.1 Hydroxy acids. The two beta‐hydroxy acids used in dermatology are SA and LHAs. Unlike the alpha‐hydroxy acids, SA is lipid‐soluble, allowing it to penetrate not only the epidermis but also the pilosebaceous unit. This added penetration makes it a comedolytic, thus giving it superiority over the alpha‐hydroxy acids in treating acne [33]. SA also exerts anti‐inflammatory effects by inhibiting arachidonic acid. Multiple studies exist demonstrating the superiority of SA to placebo or to benzoyl peroxide. One study examined 49 patients who applied either 0.5% SA or placebo twice daily for 12 weeks. Those who applied the SA had significantly reduced inflammatory papules and open comedones, but closed comedones were not diminished [34]. One of the two studies submitted to the FDA during the OTC approval phase was a 12‐week, double‐blind investigation of 180 subjects. It compared the efficacy of 2% SA solution with a vehicle solution and 5% benzoyl peroxide. Of the subjects treated with the SA, 40% showed a good or excellent response versus 5% in the vehicle group and only 2% in the benzoyl peroxide group. SA was better than either vehicle or benzoyl peroxide in improving total lesions, inflammatory lesions, and open comedones, but not closed comedones. The second study submitted to the FDA involved 187 subjects and compared 0.5% and 2% SA solution with the vehicle solution. Both 0.5% and 2% SA were superior to the vehicle in reducing inflammatory lesions, open and closed comedones, and total lesions [35]. There are also several studies that demonstrate the efficacy of SA formulations other than solution. A cross‐over study evaluating a 2% SA cleanser and a 10% benzoyl peroxide lotion in 30 patients found the SA cleanser to be superior at improving comedones [36]. Another study demonstrated the efficacy of a 2% SA scrub in reducing open comedones [37]. Based on these studies, many consider SA more effective than benzoyl peroxide in treating comedonal acne, but less effective than benzoyl peroxide in treating inflammatory acne [35]. Unlike benzoyl peroxide, SA does not have the ability to prevent resistance when used in combination with oral or topical antibiotics. There is some evidence to suggest that combination treatment with both a SA and glycolic acid may be superior to either alone in the treatment of acne [38]. A study in 2018 concluded that SA targeted two of the four pathological processes in acne: sebosuppressive and anti‐inflammatory activities. SA showed sebosuppressive properties through the downregulation of the AMPK/SREBP‐1 signaling pathway and inflammatory response through the inhibition of the NF‐kB pathway in SEB‐1 sebocytes [39]. Lipohydroxy acids (LHAs), a derivative of SA, have a similar mechanism of action. Like SA, LHAs work as an exfoliant and ketolytic agent but are more lipophilic than SA, causing them to have slower chemical reactions. This leads to gentler exfoliation and is shown to be less irritating to sensitive skin [40]. Although the FDA does not recognize LHA as a main ingredient in antiacne therapies, there is some research to support the use of LHA‐containing products in the treatment of acne. One study, using 80 subjects with mild to moderate acne were utilized to test LHA used twice a day to 5% benzoyl peroxide used once a day. At the end of the 12 weeks, there were no statistically significant differences between the two groups, both of which showed an averaged 21% decrease in inflammatory lesions [41]. Based on these results, LHA could be a milder alternative to acne treatment for patients who cannot tolerate benzoyl peroxide products. Another study of 73 participants evaluated the efficacy of SA 1.5% and LHA 0.3% twice a day to tretinoin 0.5% cream once nightly. The results of this study concluded that both SA/LHA and tretinoin were effective in reducing acne vulgaris, however were not found to be equivalent. Although tretinoin had a higher success at reducing the total number of comedones in acne vulgaris patients, the SA/LHA formula could be another treatment option for patients who are intolerant to tretinoin [42].
CHAPTER 57
Over‐the‐Counter Acne Treatments
Introduction
Soaps and syndets
Benzoyl peroxide
Alpha‐hydroxy acids
Hydroxy acid
Solubility
Source
Penetration
Action
Over‐the‐counter strength
Alpha‐hydroxy acids
Water soluble
Dermis (at high concentrations)
Exfoliative
Less than 10%
Glycolic acid
Sugar cane
Lactic acid
Sour milk
Beta‐hydroxy acids
Lipid soluble
Epidermis and pilosebaceous unit
Exfoliative, comedolytic, anti‐inflammatory
0.05–5%
Salicylic acid
Willow bark, wintergreen, sweet birch
Lipo‐hydroxy acid
Derivative of salicylic acid
Poly‐hydroxy acids
Water soluble
Dermis
Exfoliative
3–12%
Gluconolactone
Palm and coconut
12%
Lactobionic acid
Caspian Sea Yogurt
3%
Beta‐hydroxy acids
Polyhydroxy acids
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


