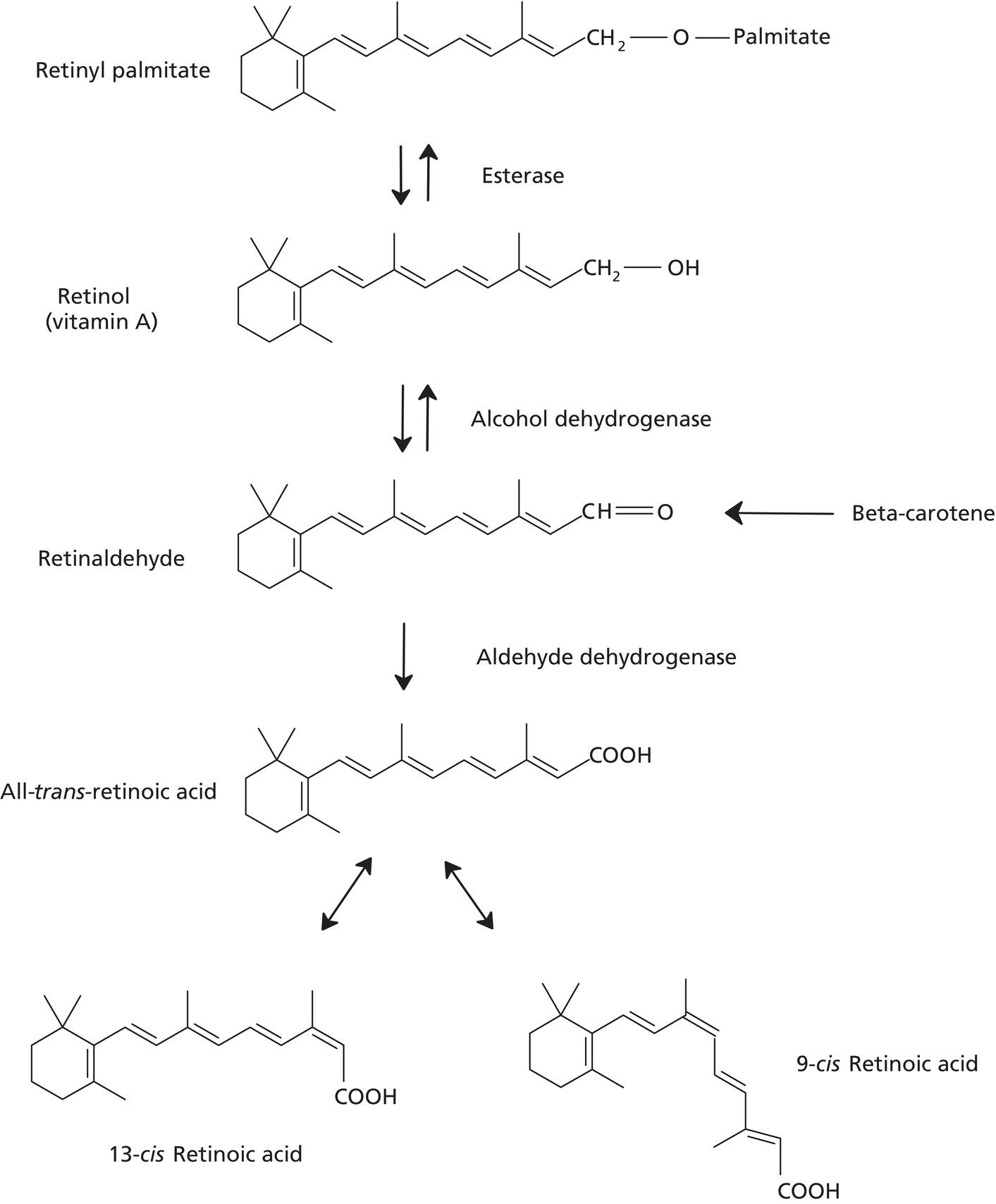
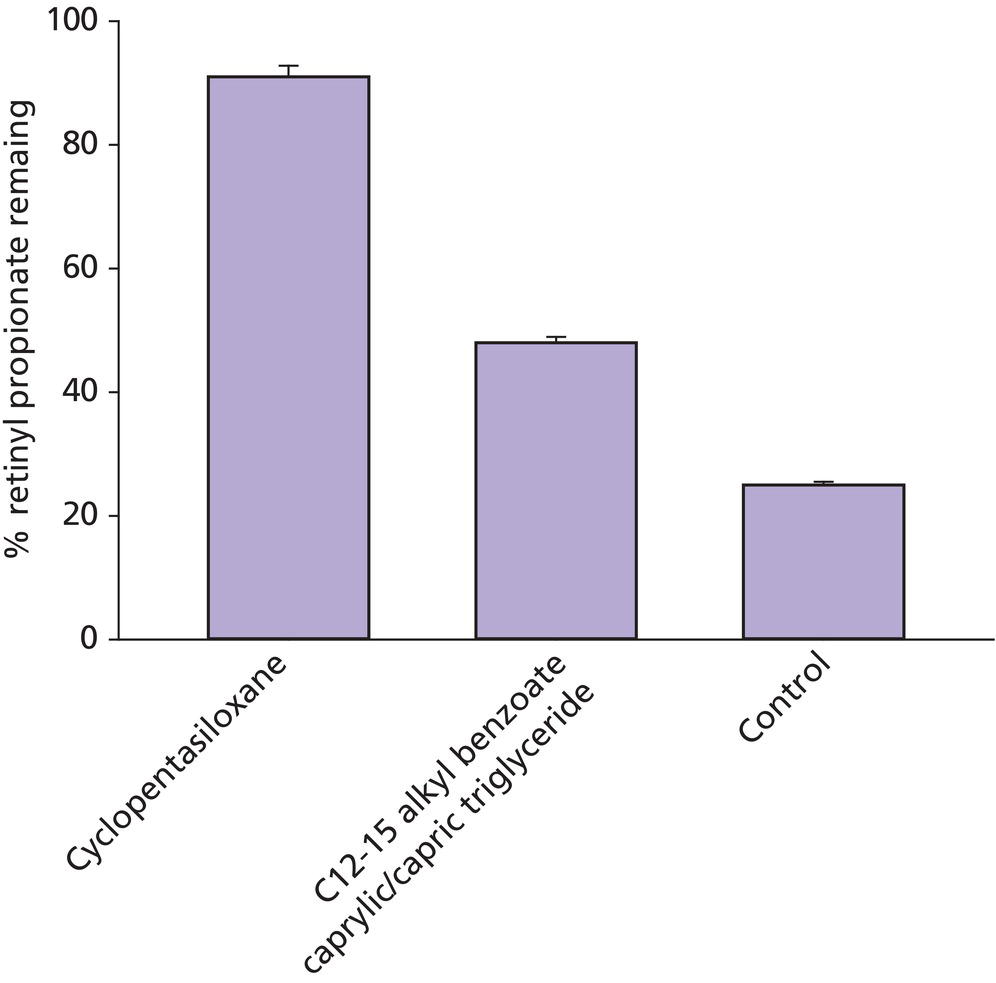
John E. Oblong and Joseph H. Jansen Procter and Gamble Beauty Science, The Procter and Gamble Co., Cincinnati, OH, USA Vitamins are organic compounds required for maintaining human health and are primarily obtained from the diet. Numerous vitamins have been utilized in topical cosmetic products based on limitations that can develop from nutrient distribution due to aging, particularly in photoaged skin. By definition, vitamins are essential nutrients and thus are involved in numerous biochemical and molecular regulatory processes. They are chemically diverse and can be classified into water‐ or oil‐soluble vitamins. Relative to skin care, they have the potential to provide beneficial effects across a wide spectrum of skin problems, even in people who are nutritionally sufficient. Also, since they have been well studied due to their importance in nutrition, the underlying mechanisms and toxicology are often well understood. Additionally, with topical application and subsequent delivery into skin, they are more likely to have an elevated localized impact in comparison to oral intake with the consequent limited delivery via the circulation to the specific skin site of interest (e.g. facial skin). This is particularly true of oil‐soluble vitamins such as vitamin A and E. Since there are numerous vitamins [1], this review is necessarily selective, focusing on a few, with particular emphasis on those materials for which there are available well‐controlled in vivo human studies to illustrate skin care effects. Selected literature citations are provided to give the reader some references that can serve as a starting point to probe deeper into the published technical data. Several forms of the oil‐soluble vitamin A are used cosmetically, the most widely utilized ones being retinol, retinyl esters (e.g. retinyl acetate, retinyl propionate, and retinyl palmitate), and retinaldehyde. Through endogenous enzymatic reactions, all are converted ultimately to trans‐retinoic acid (RA), the active form of vitamin A in skin. Specifically, retinyl esters are converted to retinol via esterase activity. Retinol is then converted to retinaldehyde by retinol dehydrogenase. Finally retinaldehyde is oxidized to RA by retinaldehyde oxidase (Figure 41.1). Since trans‐RA is the active form of vitamin A in skin, the abundant published literature on the former is applicable to this discussion. RA interacts with nuclear receptor proteins described as retinoic acid receptors (RAR) and retinoid X receptors (RXR), which can form heterodimer complexes. These complexes then interact with specific DNA sequences to affect transcription, to either increase or decrease expression of specific proteins/enzymes [2]. Using genomic methodology, work in our laboratories has found that the expression of over 1200 genes is significantly affected by topical retinoid treatment of photoaged human skin (unpublished observations). Many of these changes can be ascribed, at least on some level, as being normalization of the altered skin conditions that occur with aging (induced by both chronological and environmental influences such as chronic sun exposure). Some specific changes induced by retinoid that are likely relevant to skin appearance effects are those that result in increased production of epidermal ground substance (glycosaminoglycans or GAGs which bind water, increasing epidermal hydration); increased dermal production of extracellular matrix components such as collagen (to increase dermal thickness and restructure the matrix); and thicker and “restored” epidermis, e.g. increased epidermal proliferation and differentiation (increased epidermal thickness and epidermal turnover). These effects would be expected to contribute to improvements in the appearance of fine lines, wrinkles, and roughness [3]. Figure 41.1 Conversion of retinyl ester into trans‐retinoic acid in the skin. In addition to stimulation of events in skin, retinoids also have an inhibitory effect on other tissue components. For example, retinoids are reported to inhibit production of collagenase. While retinoids will stimulate production of ground substance (GAGs) in epidermis, they have the opposite effect in dermal tissue, specifically inhibiting production of excess ground substance in the upper dermis of photoaged skin. While a low level of GAGs is required in the dermis for normal collagen structure and function, excess dermal GAGs are associated with altered dermal collagen structure and wrinkled skin appearance in photoaged skin. Removal of the excess dermal GAGs has been shown to be associated with improved matrix structure and reduced skin wrinkling. Since at least some of the epidermal effects of topical retinoid (e.g. epidermal thickening and turnover) occur relatively rapidly (days) after initiation of treatment, some skin surface effects (e.g. diminution of roughness and fine line appearance) can potentially be realized quickly [4]. The dermal effects likely occur on a much longer time frame (weeks to months) such that reduction in skin problems via this mechanism will require much longer time frames (weeks to months). In addition to the fine line, wrinkle, and roughness effects of retinoids, they are also well known as agents to improve hyperpigmentation (e.g. hyperpigmented spots, post‐inflammatory hyperpigmentation, solar lentigos, melasma), with the effect being achievement of lighter and more uniform skin color. The mechanisms by which retinoids affect the skin’s pigmentary system have not been completely identified. Yet, it is known that retinoids stimulate epidermal turnover, which simply could be interpreted as exfoliating pigmented stratum corneum cells from the skin surface. Retinoids also inhibit ultraviolet (UV)‐induced pigmentation via reducing tyrosinase activity and melanin synthesis, by regulatory action on transcription processes in the epidermis (in melanocytes and keratinocytes) [5]. These effects would reduce hyperpigmentation, leading to lighter skin color over a time frame of at least two weeks. While much of the substantial literature on the improvement of skin fine lines, wrinkles, roughness, and hyperpigmentation by topical retinoids is focused on trans‐RA, there are also data available on the vitamin A compounds that are used cosmetically. Since retinoids are irritating to skin, defining skin‐tolerated concentrations clinically is a key step in working effectively with these materials. Retinol is better tolerated by the skin than trans‐RA. In our testing, we noted that retinyl propionate is milder to skin than the widely used retinol and retinyl acetate (Table 41.1) [6]. Table 41.1 Cumulative back irritation measures for retinol and its esters (double‐blind, vehicle‐controlled, randomized study; daily patching for 20 days, under semi‐occluded patch, n = 45; 0–3 irritation grading). Equimolar doses and abbreviations used were: 0.09% RP (retinyl propionate), 0.086% RA (retinyl acetate), and 0.075% ROH (retinol). RP and RA were significantly less irritating than ROH, and RP was directionally less irritating than RA. a Treatments with the same letter codes are not significantly different from each other (p < 0.05). Since retinoids in general tend to be fairly potent, topical doses of less than 1% are generally sufficient to obtain significant effects. At low doses, in double‐blind, split‐face, placebo‐controlled facial testing (12‐week duration), both retinol and retinyl propionate have been shown to be significantly effective in reducing facial hyperpigmentation and fine lines/wrinkles across the study (Figure 41.2). Determination of treatment effects was based on quantitative computer image analysis and blinded expert grading of high‐resolution digital images [6]. There are also clinical studies published on other retinoids. Retinyl palmitate has a very low irritation potential but is also considered to have a much lower efficacy response profile. This is due presumably to the fact that the primary storage form of retinoids in skin is the palmitate ester form. While it has been reported that retinyl palmitate can protect against UV‐induced erythema [7], to date there are no reported single variable clinical studies to show significant efficacy [8]. There are also a few studies revealing the clinical efficacy of retinaldehyde, typically at a dose of 0.05%. However, retinaldehyde has irritation potential similar to retinol [9]. Figure 41.2 Topical retinyl propionate (RP) reduces the appearance of fine lines/wrinkles. 0.2% retinyl propionate in a stable skin care emulsion system was applied twice daily for 12 weeks. Images were taken at baseline, and weeks 4, 8, and 12. There are two primary challenges in working with retinoids. One is their tendency to induce skin irritation (as noted above), which negatively affects skin barrier properties. While high doses will provide greater skin aging appearance improvement, the associated irritation tends to define an upper concentration limit where they can be used practically. The skin may have some capacity to accommodate to retinoid treatment to respond with less irritation over time, it is not completely eliminated even with long‐term use, as demonstrated by evaluation of skin barrier function. Mitigation of the irritation may be managed to some extent with appropriate formulation to meter delivery into the skin, use of retinyl esters which are less irritating than retinol (as noted above), or inclusion of other ingredients (e.g. those with anti‐irritancy or anti‐inflammatory activity) to counter this issue. Another key issue is instability, especially to oxygen and light. Thus, to ensure stability of retinoid in finished product, formulation and packaging must be done in an environment that minimizes exposure to oxygen and light. One approach to control the instability is to use a product packaging that is opaque, oxygen impermeable, and includes a small package orifice to reduce oxygen exposure once the container is opened. Another successful approach that can significantly stabilize retinyl propionate in finished product is to solubilize the retinoid in silicone‐based solvents versus traditional ester solvents (Figure 41.3). In addition, a variety of other strategies might be employed, e.g. encapsulation of the retinoid, inclusion of stabilizing antioxidants, and unit dosing. Figure 41.3 Stability of retinyl propionate formulated in cyclopentasiloxane (silicone‐based solvent) compared with C12–15 Alkyl Benzoate/Caprylic/Capric Triglyceride (ester‐based solvent) and control. Formulations were maintained at 40°C for 4 weeks to simulate accelerated stability testing conditions. Retinyl propionate levels were quantitated via Agilent Infinity 1260 HPLC using a C18 Peek Column, 250 mm × 4.6 mm. There are three primary forms of the water‐soluble vitamin B3 that have found utility in skin care products: niacinamide (aka nicotinamide), nicotinic acid (aka niacin), and nicotinate esters (e.g. myristoyl nicotinate, benzyl nicotinate). Vitamin B3 serves as a precursor to a family of endogenous enzyme co‐factors (Figure 41.4), specifically nicotinamide adenine dinucleotide (NAD +), its phosphorylated derivative (NADP+), and their reduced forms (NADH, NADPH). NADPH/NADP+ ratios serve as an indicator of redox status whereas NAD+/NADH ratios function as a critical co‐factor in the regulation of metabolism, epigenetics, and circadian rhythms [10, 11]. Relative to vitamin deficiencies that are linked to skin health, vitamin B3 deficiency leads to the medical condition pellagra, which encompasses a broad range of symptoms from dermatitis to dementia to death [12]. These co‐factors are involved in many enzymatic reactions in the skin, and thus have potential to influence many skin processes as well as overall aging [13]. The ability of niacinamide to incorporate into cellular NAD+ pools and be utilized by sirtuins and poly‐ADP ribose polymerases may be a key mechanistic basis for the diversity of clinical effects observed for a simple material such as niacinamide [14–16]. Recently, it has been reported that niacinamide can protect both glycolysis and oxidative phosphorylation under conditions of hydrogen peroxide‐induced oxidative stress, which mechanistically involves incorporation into cellular NAD+ pools [17]. The evolving role of NAD+ in protecting cellular bioenergetics under oxidative stress conditions can be viewed as an example of how niacinamide and NAD+ pools play a significant role in maintaining skin homeostasis (oblong). Particularly, since it is known that niacinamide is a known NAD+ precursor and NAD+ levels decrease with age in skin [18]. Restoring NAD+ with niacinamide may contribute to the specific actions of niacinamide that have been reported [19–21]. For example, topical niacinamide has the following effects:
CHAPTER 41
Topical Vitamins
Introduction
Vitamin A
Forms
Mechanisms
Topical effects
Topical treatment (oil‐in‐water emulsions)
Expert grader cumulative irritation scores
Significance of expert grader cumulative scores a
Chromameter “a” measure (day 21)
Significance of chromameter “a” measure a
Emulsion control
3.9
a
0.4
a
0.09% Retinyl propionate
24
b
2.7
b
0.086% Retinyl acetate
39
b
3.8
bc
0.075% Retinol
164
c
7.6
d
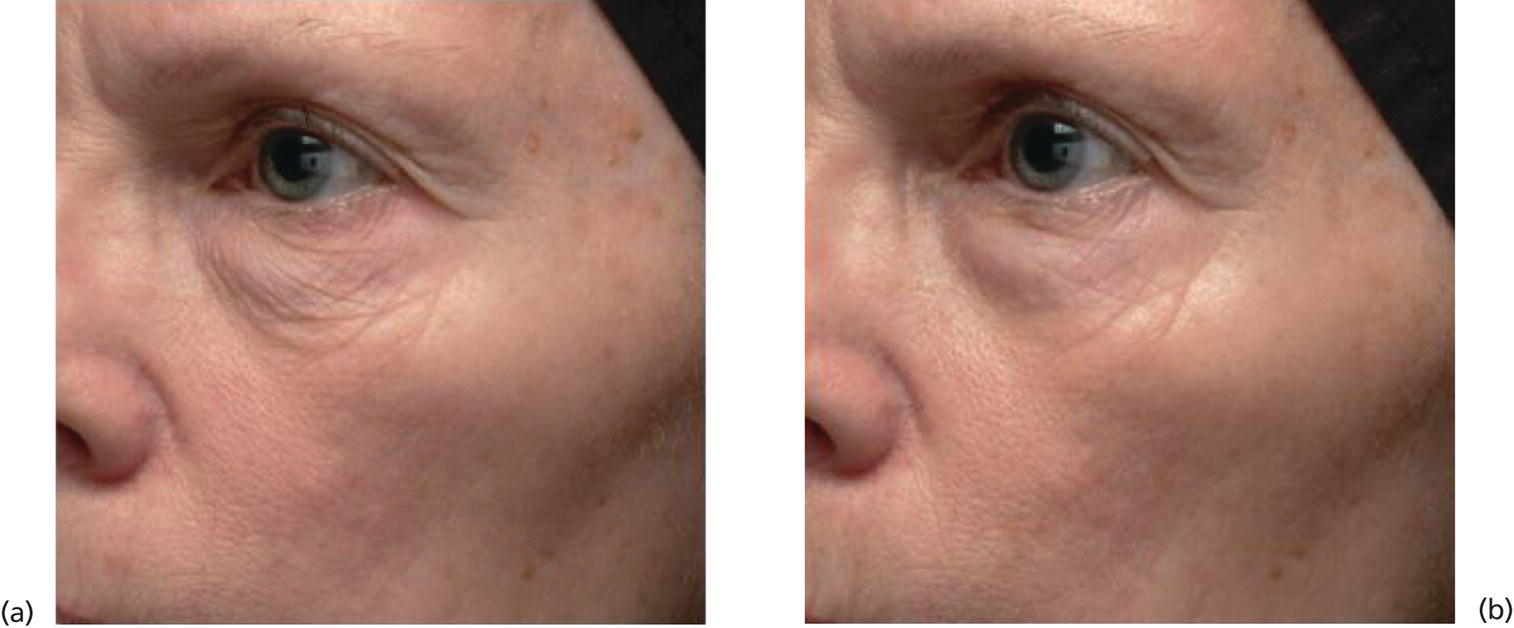
Formulation challenges
Vitamin B3
Forms
Mechanisms
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


