56. Gynecomastia
Indications and Contraindications
Typically, neonatal and pubertal cases resolve with expectant management. 1
Neonatal cases: Resolved within several weeks
Pubertal cases: 75% of cases resolved within 2 years without treatment 2
Drug-related cases can resolve with removal of the offending agent before the development of breast tissue fibrosis.
Pathological causes necessitate formal medical evaluation with special attention to the associated comorbidities.
Patients with Klinefelter syndrome (karyotype 47, XXY) have a 50× higher incidence of male breast cancer. (The prevalence of Klinefelter syndrome in males with breast cancer is 7.5%.) 3 , 4
The presence of hypertrophic breast tissue for >12 months typically warrants surgical treatment because of fibrotic transformation. 5 , 6
Demographics
Etiologic factors
Often multifactorial, involving excess estrogens, decreased androgens, and/or androgen receptor defects.
Clinical classes
Idiopathic: Most common (25%)
Physiologic
Neonatal: Influence of maternal estrogens
Pubertal: Elevated estradiol/estrogen ratio
Senile: Peripheral conversion of testosterone to estrogen by aromatase
Pathological: Cirrhosis, kidney failure, testicular/adrenocortical/pituitary tumors, hypogonadism, hyperthyroid, adrenal hyperplasia, and bronchogenic carcinoma
Pharmacologic: Estrogens, gonadotropins, androgens, antiandrogens, chemotherapy agents, calcium channel blockers, ACE inhibitors, digitalis, CNS agents, antituberculosis medications, and drugs of abuse
Histology
Represents the cellular changes seen with prolonged gynecomastia
Florid: Symptoms <4 months; cellular stroma and ducts increased
Intermediate: Symptoms present 4-12 months; mix of florid and fibrous patterns
Fibrous: Gynecomastia present >1 year; minimal ducts but extensive stromal fibrosis
Preoperative Evaluation
History
Age of onset
Duration
Additional symptoms
Current/recent medications
Illicit drug use
Past medical history
Family history (breast cancer)
Senior Author Tip:
Be certain to note whether or not the presence of the excess breast tissue causes pain. This can be an important symptom that may determine whether or not insurance coverage will be extended for treatment.
Physical Examination
Breast: Fatty versus fibrosis, ptosis grade, masses, skin excess, unilateral versus bilateral, milky discharge (prolactin-secreting tumor)
Testicular examination: Size, masses, firmness
Ultrasound examination for abnormal findings (i.e., masses)
Organomegaly: Liver, thyroid, abdominal viscera
Feminine features
Absence of masculine attributes (i.e., hair pattern)
Laboratory Tests
Beta-human TSH/free thyroxine, chorionic gonadotropin, follicle-stimulating hormone, luteinizing hormone, serum testosterone, and estradiol levels to correlate abnormal physical findings
Consider liver function tests for hepatomegaly.
Endocrine consult and chromosomal analysis when indicated
Imaging
Breast imaging through mammography or ultrasonography: May be controversial, because gynecomastia is much more common than male breast cancer
Mammography: When breast cancer is suspected. 9 Helpful for assessing the quality of breast tissue (fatty versus fibrous)
Tip:
Completion of a testicular exam needs to be documented in the medical record. If there is any concern for potential scrotal mass or inconsistency in testicular exam, ultrasound imaging of the scrotum/testicles is indicated.
Staging
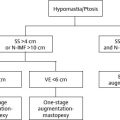
Grade I: Minimal hypertrophy (<250 g) and no ptosis
Grade II: Moderate hypertrophy (250-500 g) and no ptosis
Grade III: Severe hypertrophy (>500 g) and grade I ptosis
Grade IV: Severe hypertrophy (>500 g) and grade II or III ptosis
Informed Consent
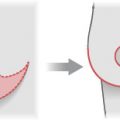
If surgery is indicated, the planned incisions and appearance are discussed.
Pictures/diagrams are used to reinforce the discussion.
Both the general and the most relevant potential complications (see preceding section) are included.
Asymmetry, contour irregularities, and the need for further procedures are discussed, especially when liposuction is used alone or staged excision is planned.
Technique
Nonoperative
Expectant management is recommended for neonatal (weeks to months), pubertal (up to 2 years), and idiopathic cases.
Offending agents (medications, drugs) are removed or changed if pharmacologic source suspected.
Hormonal therapy is considered where appropriate.
Testosterone, antiestrogens (tamoxifen), and danazol show limited efficacy.
For pathological causes, the underlying disease or source (i.e., testicular tumor; liver, pituitary, or thyroid disease) is treated.
Gynecomastia present for >12 months typically will not spontaneously regress because of dense fibrosis and hyalinization.
Operative
Senior Author Tip:
If at any time the condition begins to adversely affect the normal social development of the patient resulting in social withdrawal, avoidance of normal sports activities, or embarrassment in situations where the chest is exposed as in swimming, a low threshold for operative treatment should be instituted.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


