54. Augmentation-Mastopexy
General Principles
Augmentation-mastopexy is a technique used to simultaneously correct low volume and skin excess.
Augmentation alone corrects relative deficiency of volume.
Mastopexy alone corrects relative excess of skin.
If volume deficiency and skin excess are significant enough that either procedure alone will result in a persistent relative mismatch, combined procedure is needed.
The revision rate is high (8%-20%). 1 – 3
Gonzales-Ulloa 4 described the technique in 1960, followed by Regnault 5 in 1966.
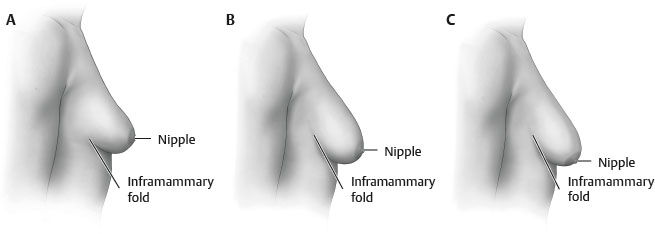
Surgical planning depends on relative locations of nipple and inframammary fold (IMF) (i.e., ptosis). Regnault described three categories67 (Fig. 54-1):
Grade I: Nipple at IMF
Grade II: Nipple below IMF
Grade III: Nipple at the lowest point on breast
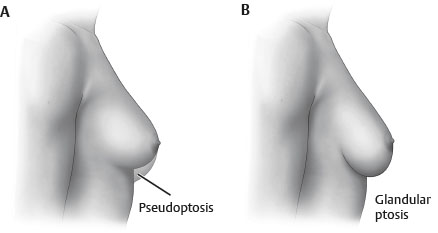
Pseudoptosis: Nipple at or above IMF but breast parenchyma below IMF 8 (Fig. 54-2, A)
Glandular ptosis: Excess gland in the lower pole of the breast 8 (Fig. 54-2, B)
Alternatives
Augmentation Alone
Use if skin excess is minimal: i.e., minimal gland below IMF, minimal ptosis, AND
Augmentation alone can provide appropriate projection and adequately correct ptosis by decreasing relative skin excess.
Mastopexy Alone
Use if volume deficiency is minimal, AND
Skin resection alone will appropriately raise the nipple position and adequately correct projection by decreasing relative volume deficiency.
Indications
Ptosis (skin excess) combined with significant volume deficiency
Periareolar mastopexy with augmentation requires 9 :
Nipple no more than 2 cm below the fold
Nipple-areola complex (NAC) at or above breast border, not pointing inferiorly
No more than 3-4 cm of associated breast ptosis
More significant ptosis will require a vertical or Wise-pattern mastopexy.
Single-Stage Versus Two-Stage Procedure
Single-Stage Procedure
Thought to be unpredictable, with higher revision rate than that of both procedures combined 11
One of the most common causes for malpractice claims 12
Constricted breast or skin deficiency
Unclear whether both procedures will be necessary
For example, no mastopexy required if patient has 13 :
No ptosis and no pseudoptosis (<2 cm of breast parenchyma below the IMF)
Alternatively, per Lee, Unger, and Adams, 15 skin stretch <4 cm and nipple-to-IMF (N-IMF) distance <10 cm
Significant asymmetry that is going to require an asymmetrical mastopexy for correction
Significant vertical skin excess that will require a large skin resection
Two-Stage Procedure
Per Lee, Unger, and Adams, 15 vertical excess >6 cm is indication for staging procedure.
If primary goal is ptosis correction, perform mastopexy first, and stage augmentation.
If primary goal is improved projection or upper pole fullness, place implant first, and stage the mastopexy.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


