53. Mastopexy
Natural History and Classification
Breast Changes: Multifactorial
The amount of breast parenchyma changes with age, body weight, pregnancy, and hormonal changes.
The skin envelope is stretched when the parenchyma enlarges.
Supporting ligaments and ductal structures are also stretched.
Ptosis results when the parenchymal volume decreases, and the skin envelope and supporting structures do not retract.
As a consequence, the breast assumes a lower position on the chest wall, and the youthful breast contour is lost.
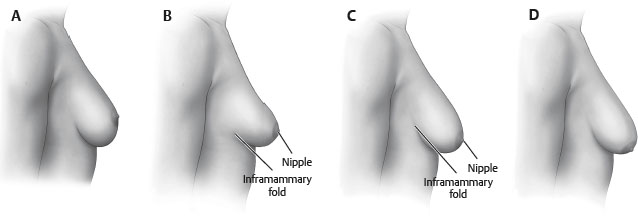
Regnault Classification
Describes ptosis by the relative position of the nipple-areola complex (NAC) and the inframammary fold
Grade I ptosis (mild ptosis)
NAC is at the level of the inframammary fold.
Grade II ptosis (moderate ptosis)
NAC lies below the level of the inframammary fold, but remains above the most dependent part of the breast parenchyma.
Grade III ptosis (severe ptosis)
NAC lies well below the inframammary fold and at the most dependent part of the breast parenchyma along the inferior contour of the breast.
Pseudoptosis or glandular ptosis
NAC is above or at the level of the inframammary fold, but most of the breast parenchyma has descended below the level of the fold.
Nipple-to-inframammary fold distance has increased.
Indications and Contraindications
Indications
Women who desire an improvement in breast contour without a change in volume
Women who seek a more lifted, “perky,” youthful breast appearance and aim to correct upper pole deflation, ptosis of the areolar complex and breast tissue, and laxity of skin envelope
Contraindications
Active smoking
Women who desire volume change
Preoperative Evaluation
History
Age: Involution of breast after menopause
Breast history: Lactation, pregnancy changes, size changes with weight loss/gain, tumors, previous procedures, family history of breast cancer, recent mammogram
Patient goals
Medications, including psychotropic, oral contraceptive, and hormone replacement 6
Measurements
Sternal notch-to-nipple distance: Allows detection of asymmetry in nipple position
Nipple-to-inframammary fold distance: A measurement of the redundancy of the lower pole skin envelope
Classification of ptosis severity (see Fig. 53-1)
Other Considerations
Breast position on chest wall: Patients with low breast position without significant ptosis will not benefit from mastopexy. 7
Skin quality and amount: Presence of striae reflects the inelastic quality of affected skin; degree of skin laxity
Parenchymal quality: Fatty, fibrous, or glandular parenchyma and overall volume
Areolar shape and size: Areola are often stretched and large with asymmetries.
Photographs
AP, lateral, and oblique photographs should be obtained (see Chapter 3).
Patient Expectations
Breast size
Mastopexy techniques combine small amounts of parenchymal resection (<300 g traditionally in literature 3 ) and redistribution with reduction of the skin envelope — this can result in a reduction in breast size.
Average decrease of one cup size postoperatively: Important in patient counseling. 3
Many patients desire restoration of upper pole fullness, which may necessitate the placement of an implant simultaneously.
Mastopexy, augmentation-mastopexy, and reduction all increased breast and upper pole projection with significantly greater boost when implants were combined with mastopexy. 8
Volume-deficient patients may often require augmentation-mastopexy as well 7 (see Chapter 54).
Scar position
Mastopexy procedures trade scars for improved contour.
Patients should be informed in detail preoperatively about scar placement and scar quality.
Other considerations
Thorough patient education regarding procedural complications, use of drains, and recurrence of ptosis are essential components of preoperative preparation.
Informed Consent
Recommend items to be included in the informed consent:
A general description of the procedure and location of incisions and the potential need for placement of drains
A sufficient description of potential risks
Bleeding and hematoma
Infection
Delayed healing and wound separation
Change in nipple and skin sensation
Potential changes in breast-feeding
Asymmetry and poor cosmetic result
Poor scar quality
Tip:
Postoperative scars are a frequent source of litigation; therefore they are an essential component of the informed consent process. However, breast shape should not be compromised to reduce the scar burden.
Mastopexy Techniques
Historically, mastopexy was based on primary skin excision; however, since the mid-1990s, internal shaping of tissue using various supportive materials or parenchymal pillars has also been emphasized. 4
Technique depends on degree of ptosis.
Periareolar Techniques
General
Incisions are made and closed around the areola.
Scars are therefore camouflaged at the areolar-skin junction.
Patient Selection
Useful with mild and moderate ptosis
Skin quality should be reasonable without striae, and parenchyma should be fibrous or glandular.
Techniques
Simple periareolar deepithelialization and closure
Breast parenchyma is not repositioned; therefore only useful with mild ptosis
Permits nipple repositioning
Limited ellipitical techniques can elevate the NAC approximately 1-2 cm. 2
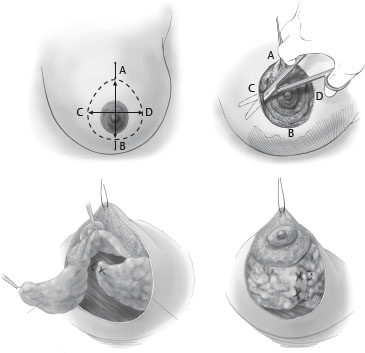
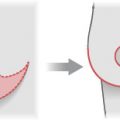
Benelli technique 9 (Fig. 53-2)
A periareolar technique that can be applied to patients with larger degrees of breast ptosis
Allows parenchymal repositioning
Areolar sizers are used to mark the new areolar diameter, and a wider ellipse is marked to reposition the NAC and resect redundant skin envelope.
Undermining separates the breast gland from the overlying skin.
The breast parenchyma is then incised leaving the NAC on a superior pedicle.
Medial and lateral parenchymal flaps are mobilized and crossed or invaginated in the midline, narrowing the breast width and coning the breast shape.
The periareolar incision is closed in a purse-string fashion with permanent suture.
Other periareolar techniques
Advantages
Short scar
Scar position camouflaged at border of pigmented areola and nonpigmented skin
Disadvantages
Scar and areolar widening occur frequently.
Breast projection can be flattened.
Purse-string closure results in skin pleating that takes several months to resolve.
Senior Author Tip:
If periareolar purse-string suture remains palpable, it can be removed in a simple office-based procedure after 6 weeks.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


