51. Breast Anatomy
Embryology, Development, and Physiology
Embryology
The breast is ectodermally derived.
From week 8-10 of embryologic development, breast growth begins with differentiation of cutaneous epithelium of pectoral region.
In week 6, milk ridge develops extending from axilla to groin.
From week 7 of gestation to birth, mammary anlage on chest wall develops into an epithelial bud with 15-20 ducts, and nipple develops into circular smooth muscle fibers.
First 7 weeks after birth, clear fluid similar to colostrum (“witch’s milk”) containing water, fat, and cellular debris may be secreted from the neonatal breast, stimulated by maternal hormones.
Normal breast development in anterolateral pectoral region at level of fourth intercostal space
Supernumerary breasts (polymastia) and nipples (polythelia) can occur along milk ridge.
Most common location for polymastia is lower left chest wall below the inframammary crease.
Polythelia is the most common congenital breast anomaly, occurring in 2% of the population.
Abnormal regression of milk line can lead to underdevelopment of breasts (hypoplasia).
Complete absence of breast (amastia) usually associated with hypoplasia of ipsilateral pectoralis musculature and chest wall (Poland syndrome).
Development
Puberty begins at 10-12 years of age as a result of hypothalamic gonadotropin-releasing hormones secreted into the hypothalamic-pituitary portal venous system.
Anterior pituitary secretes follicle stimulating hormone (FSH) and luteinizing hormone (LH).
FSH causes ovarian follicles to mature and secrete estrogens.
Estrogens stimulate longitudinal growth of breast ductal epithelium.
As ovarian follicles become mature and ovulatory, the corpus luteum releases progesterone, which, in conjunction with estrogen, leads to complete mammary development.
Stages of breast development described by Tanner 1 :
Stage 1: Preadolescent elevation of nipple only; no palpable glandular tissue or areolar pigmentation
Stage 2: Presence of glandular tissue in the subareolar region; nipple and breast project as single mound
Stage 3: Further increase in glandular tissue with enlargement of breast and nipple but continued contour of nipple and breast in single plane
Stage 4: Enlargement of areola and increased areolar pigmentation with secondary mound formed by nipple and areola above level of breast
Stage 5: Final adolescent development of a smooth contour with no projection of the areola and nipple
Normal variants in breast development
Infantile hyperplasia of breast
Result of transplacental estrogen from maternal-placental unit
Occurs in both sexes and may be associated with secretion of colostrum
Found in more than half of newborns
Pubertal gynecomastia
Occurs in 70% of boys
May be unilateral or bilateral
Tender
Can persist for up to 2 years
Premature thelarche
Breast development beginning before 8 years of age in girls without other signs of puberty or skeletal maturation
Most often bilateral but can be unilateral
Usually noted with first 2 years of life and ends after 3-5 years
Delayed maturation
Absence of breast development by 14 years of age in absence of chronic illness or endocrine abnormality
Family history of delayed maturation typical
Because relatively uncommon, need to rule out primary ovarian failure by testing for abnormal gonadotropin levels
Menstrual Cycle
Premenstrual: Estrogen peak, breast engorgement, breast sensitivity
Follicular phase (days 4-14): Mitosis and proliferation of breast epithelial cells
Luteal phase (days 5-28): Progesterone levels rise, mammary ducts dilate, and alveolar epithelial cells differentiate into secretory cells; estrogens increase blood flow to breast
Menstruation: Breast involution and decrease in circulating hormones
Breast engorgement and tenderness (at a minimum 5-7 days after menstruation): Palpation is most sensitive for detecting masses and most comfortable for patient at this time.
Pregnancy and Lactation
Marked ductal, lobular, and alveolar growth occurs under influence of estrogen, progesterone, placental lactogen, prolactin, and chorionic gonadotropin.
First trimester: Estrogen influences ductal sprouting and lobular formation, early to late breast enlargement ensues, superficial veins dilate, and pigmentation of nipple-areola complex (NAC) increases.
Second trimester: Lobular events predominate under influence of progestins, and colostrum collects within the lobular alveoli.
Third trimester: By parturition, breast size triples from vascular engorgement, epithelial proliferation, and colostrum accumulation.
Withdrawal of placental lactogen and sex hormones with delivery results in breast being predominantly influenced by prolactin.
Anterior pituitary secretion of prolactin influences milk production and secretion.
Posterior pituitary secretion of oxytocin leads to breast myoepithelial contraction and milk ejection.
Prolactin and oxytocin secretion is stimulated by nursing infant’s tactile stimulation of nipple.
Postlactational involution occurs during the 3 months after cessation of nursing; regression of extralobular stroma is a primary feature.
Menopause
Involves loss of glandular tissue and replacement with fat
Some lobules remain, but postmenopausal breast consists mainly of fat, connective tissue, and mammary ducts.
Vascular Supply
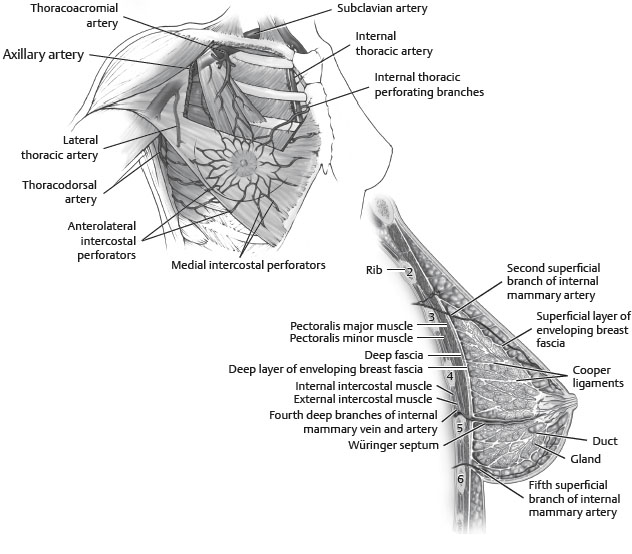
Arterial Supply
Skin
Receives blood supply from subdermal plexus, which communicates through perforators with underlying deeper vessels supplying the breast parenchyma.
Parenchyma
Supplied by:
Perforating branches of internal mammary artery
Lateral thoracic artery
Thoracodorsal artery
Intercostal perforators
Thoracoacromial artery
Nipple-areola complex
Receives both parenchymal and subdermal blood supply
Venous Drainage
Follows the arterial supply
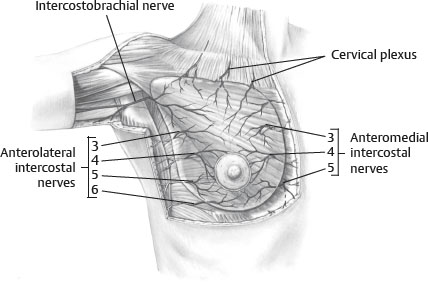
Innervation
Dermatomal in nature
Derived from the anterolateral and anteromedial branches of the thoracic intercostal nerves T3-5
Supraclavicular nerves from lower fibers of cervical plexus also provide innervation to the upper and lateral portions of the breast.
Nipple-areolar sensation is derived from the anteromedial and anterolateral T4 intercostal nerve.
Intercostal brachial nerve courses across axilla to supply upper medial arm and is often injured during axillary dissection, resulting in anesthesia and paresthesia.
Anatomic Studies
Schlenz et al 3
28 unilateral breast dissections in female cadavers
Found consistent innervation of the NAC by the anterior and lateral cutaneous branches of the third through fifth intercostal nerves
Lateral cutaneous branch (LCB) supplied innervations through posterior innervations of the nipple in 93%.
Fourth LCB provided posterior innervations in 93% of cases and was the only source 79% of the time.
Anterior cutaneous branch (ACB) had superficial course to supply medial aspect of NAC.
Third and fourth ACB combined to provide innervations in 57% of cases.
28 anatomic dissections and 14 arterial injection studies of female cadavers
Defined a “brassierelike” connective tissue suspensory system
Found neurovascular supply to the nipple runs along this well-defined suspensory apparatus
Vertical ligaments originated from the pectoralis minor (laterally) and sternum (medially)
Defined parenchymal borders and carried corresponding neurovascular structures
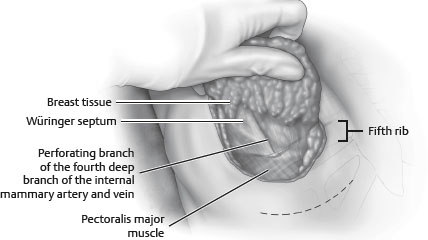
Horizontal septum originated from the pectoral fascia along the fifth rib: Würinger septum (Fig. 51-3).
It merged with the lateral and medial vertical ligaments.
Breast parenchyma was bipartitioned as the septum ran anteriorly to the NAC.
Cranial aspect carried thoracoacromial and lateral thoracic arterial branches.
Caudal aspect carried branches of the fourth through sixth intercostal arteries.
Main contributory nerve to the nipple (LCB of fourth intercostal) was always found within septum.
O’Dey et al 6
Injection study of seven female cadavers with arterial distribution patterns mapped for 14 breasts
Outlined four distinct arterial zones
Largest territory supplied by branches of the internal mammary (zone 1) and lateral thoracic (zone 2)
Evaluated safety of eight different pedicles based on vascular reliability and regularity to the NAC
Concluded that pedicles with a lateral or medially based component may be safer strictly based on regularity of arterial anatomy
Study did not account for added safety with greater breast width.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


