5 Functional and Aesthetic Genital Surgery in the Male
5.1 Fundamentals
5.1.1 Anatomy
The external male genitals include the penis and scrotum. The penis can be divided into three sections:
Root.
Body.
Glans.
The root of the penis anchors the proximal penis to the bony pelvis. This fixation is essentially ensured by the fundiform ligament of the penis from the linea alba of the fascia of the abdominal wall and the suspensory ligament of the penis from the inferior margin of the pubic symphysis as well as the bulbospongiosus and ischiocavernosus muscles. The two diverging penile crura and the bulb of the penis also lie in the region of the penis root.
Separated from each other by the pectiniform septum, the two corpora cavernosa of the penis lie on the dorsum in the body of the penis. Beneath them in the center lies the corpus spongiosum, which surrounds the urethra. The corpora cavernosa are invested in a capsule of connective tissue approximately 1 mm thick and are known as the tunica albuginea. The coronary groove represents the junction between the body and the glans of the penis.
The glans of the penis contains the corpus spongiosum of the glans, the continuation of the corpus spongiosum of the proximal penis. The external orifice of the urethra (urethral meatus) is located at the distal end of the glans. The entire length of the penis is invested in the deep fascia of the penis (Buck’s fascia), which lies superficial to the tunica albuginea. The superficial dartos or Colles’ fascia of the penis lies superficial to the Buck’s fascia beneath a mobile layer of skin forming a fold on the glans, the foreskin (or prepuce of the penis). The average penis is 7 to 10 cm long in the flaccid state and 12 to 18 cm long when erect. The average circumference is 9 to 13 cm.
The scrotum is located in the genital region between the legs, penis, and perineum. The scrotum is a multilayer sac of skin and is divided into two compartments by the scrotal septum. Each half contains a testis, epididymis, parts of the vas deferens, and the end of the spermatic cord. The internal pudendal artery and its branches supply the penis. Venous drainage in the deep layer is provided by the deep dorsal vein of the penis, which opens into the prostatic venous plexus or the internal pudendal vein. The region is drained superficially by the superficial dorsal veins of the penis, which course between the Colles fascia and Buck’s fascia. They, in turn, drain into the external pudendal veins or the femoral vein.
5.1.2 History and Preoperative Preparations
Although functional and aesthetic surgery on the male member has gained popularity since it was first described in the early 1900s and many surgeons have contributed to the development of the respective methods, this surgery still has a negative image. This is primarily due to the fact that the desire for seeking surgical enhancement often reflects a narrow, phallocentric understanding of masculinity.
Note
In evaluating the case, it is crucial to ascertain whether a surgical procedure can fulfill the expectations expressed by the patient. At the same time, one should be alert to the presence of a disorder of physical dysmorphism or to a personality disorder.
If the patient’s desires can be realized with the surgical means available, then the next step is to document preoperative findings in photographs with length and circumference measurements and to perform a thorough physical examination. Depending on the type of intervention planned, it is also recommended to exclude hormonal disorders and obtain ultrasound studies of the kidneys, bladder, and penis. Smears obtained from the foreskin and perineum are helpful in effectively treating possible postoperative infections.
5.2 Phalloplasty
Regardless of the significance ascribed to penis length and thickness in general, it should be remembered that a phalloplasty cannot augment the length of the penis as such but only the visible portion of it. The length increase gained by lengthening phalloplasty is only visible in the flaccid state and not in an erection, whereas the increase in an augmentation phalloplasty is visible in both the flaccid and erect states. This difference must be made clear to each patient preoperatively to address false expectations as early as possible. At the same time, the first consultation gives the surgeon an initial impression of the patient’s general physical and emotional health as well as an impression of the quality of the penoscrotal and suprapubic tissue.
The incision and extent of the division of the suspensory ligament of the penis are important for lengthening phalloplasty. After the operation, the elongation of the body, wound care, hygiene, and preoperative and postoperative photo documentation play an important role.
Caution
Just as the transverse infrapubic incision can lead to serious injuries to the lymph and blood vessels of the penis, the infrapubic V-Y plasty can be associated with extensive and occasionally deforming scars.
The increase in penis circumference achieved by an augmentation phalloplasty is a genuine gain with permanent results. Here, too, the postoperative result depends on the factors mentioned above. The success of the operation and the sustainability of this success depend significantly on the surgical method.
Particular caution is required with autologous fat grafts. Liquid accumulations of fat can lead to skin indentations that result in an umbrella-like foreskin or other deformities causing erectile dysfunction and problems during intercourse (see Chapter 2.1.3, Fillers and Lipofilling in Genital Surgery).
The same thing was observed with the use of hyaluronic acid preparations. This was accompanied by irregularities and pain due to granulomas.
Caution
The subcutaneous injection of liquefied Vaseline or silicone practiced by lay persons can cause dangerous deformations and can eventually lead to loss of the skin of the penis or of the entire penis itself.
Although implantation of an acellular collagen matrix is acceptable, it is often associated with an unnatural hardness that can cause stabbing pain during sexual intercourse.
Note
Patients of light to medium weight without massive suprapubic fat deposits are generally suitable candidates for lengthening phalloplasty.
5.2.1 Lengthening Phalloplasty
Surgical Procedure
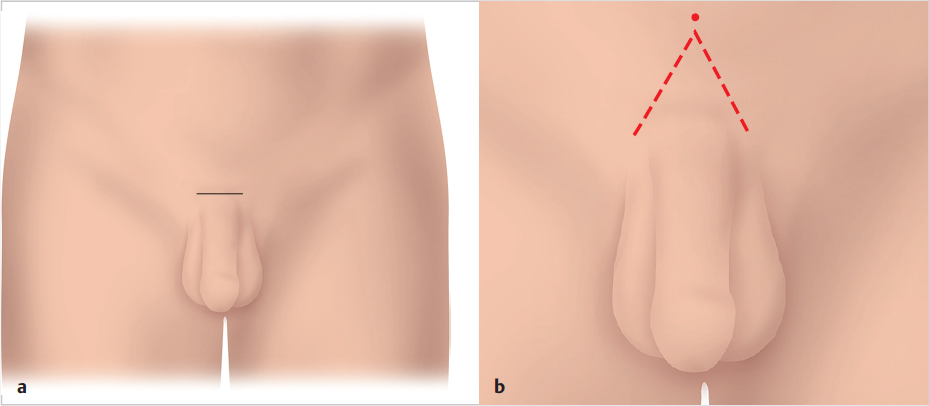
When the approach is via a transverse infrapubic incision about 3 cm long (▶Fig. 5.1a), it is possible that when the suspensory ligament is divided and the penis slides forward, the penis skin may pull back. If this withdrawal is to be reduced, using a V-Y flap is recommended instead (▶Fig. 5.1b).
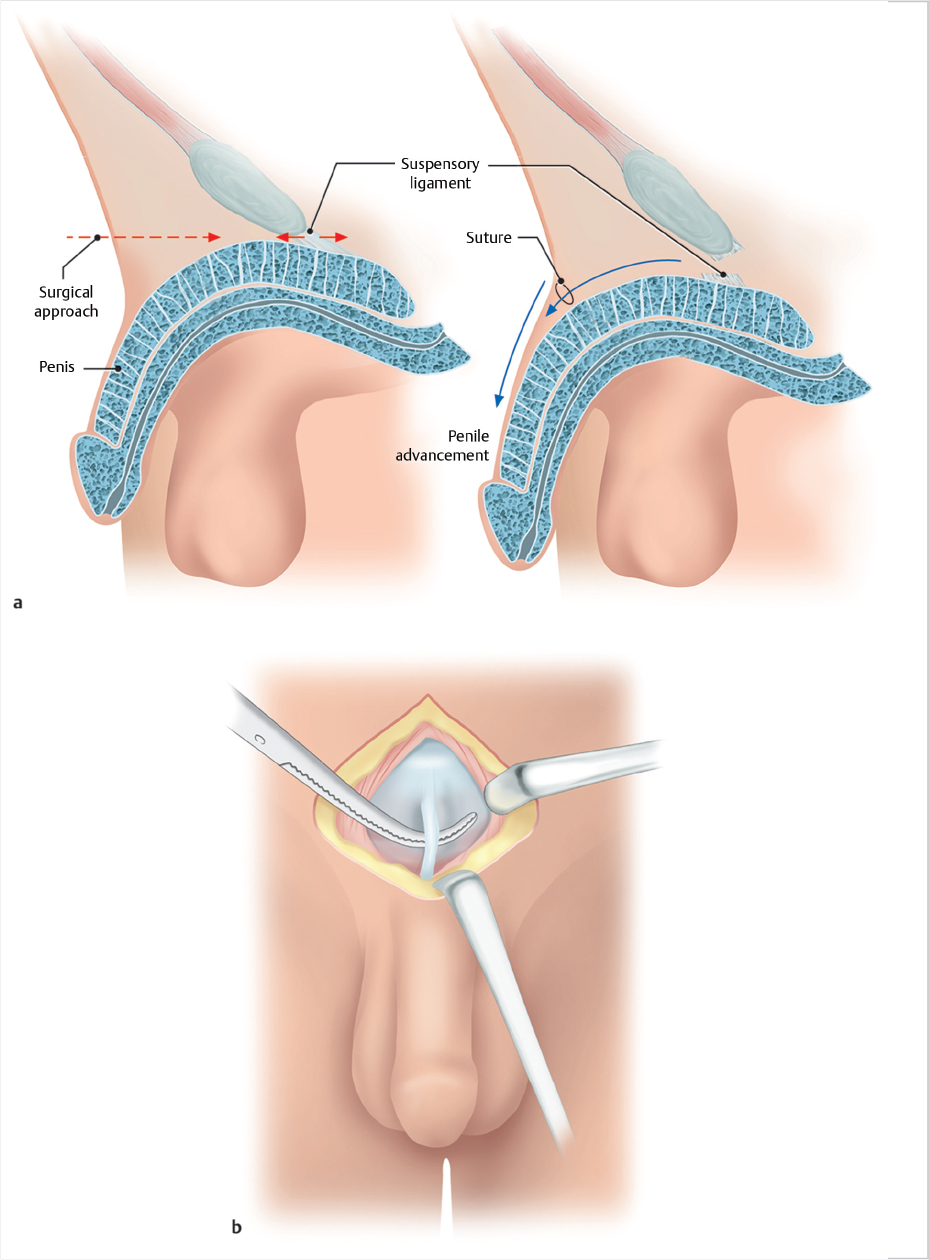
The subsequent dissection spares the bilateral superficial dorsal arteries of the penis. The superficial dorsal vein of the penis is ligated, and the Buck’s fascia is incised longitudinally. Along the corpora cavernosa, the suspensory ligament of the penis is th en exposed (▶Fig. 5.1).
Before it is divided, the bilateral vascular branches coursing through the surrounding fatty tissue must be coagulated. Then, the suspensory ligament can be exposed by blunt dissection and the spermatic cords on either side can be held back with a Roux retractor. The ligament is divided with sturdy blunt-tipped scissors close to the symphysis down to the deep fascia where the two crura of the corpora cavernosa diverge (▶Fig. 5.2a, b).
Caution
Deeper division of the ligament poses a risk of severe bleeding due to injury of the prostatic venous plexus of Santorini.
The penis has now been shifted anteriorly. To prevent it from gliding back, the tunica albuginea of the root of the penis is fixed to the skin with simple interrupted sutures (▶Fig. 5.3a, b). The proximal penis can be further emphasized by moving back the junction of the scrotum on the ventral penis. This is done by anchoring the scrotal raphe to the tunica albuginea of the penis with a simple suture (e.g., with 2–3 Vicryl) placed through a small skin incision. The suture should be placed at the lowest point of the penoscrotal fold. Alternatively, a crescentic excision of the skin fold is performed, after which the wound edges are sutured to the tunica albuginea. In selected cases, a scrotum lift is performed (see Chapter 5.3, Scrotum Lift (▶Fig. 5.3c).

Aftercare
First the body of the penis is wrapped in compresses. These are fixed in placed with hypoallergenic adhesive tape. Then a bandage under tension toward the thigh is applied with another piece of adhesive tape to prevent strangulation of the penis. This tension should be maintained for 7 to 10 days as otherwise adhesions in the region of the penis root could develop and later impair erectile function. At the same time, this prevents the penis from gliding back into its original position and negating the desired lengthening.
Complications
The medically relevant complications include:
Severe bleeding, especially due to injury of the prostatic venous plexus of Santorini or the corpora cavernosa.
Postoperative bleeding.
Severe swelling (▶Fig. 5.3d).
Hematoma (▶Fig. 5.3f).
Impaired wound healing.
Local infections.
Bleeding, postoperative bleeding, and hematoma can be avoided if careful hemostasis is achieved during the procedure and the patient observes the rules for proper postoperative behavior. Postoperative hematoma or edema will not usually require further surgical therapy and will resolve under conservative treatment. Impaired wound healing and wound dehiscence are usually superficial. They are treated conservatively. A scar contracture can occur as a secondary complication.
5.2.2 Penis Augmentation
Surgical Procedure
Patients of light to medium weight without massive suprapubic fat deposits are generally good candidates for penis augmentation. Obese patients and patients with a buried penis are not suitable for penis augmentation.
The procedure usually begins with the patient in a prone or lateral position to facilitate harvesting a free adipocutaneous graft from the gluteal fold. The size of the graft depends on the respective findings. As a general rule, three strips, each 1 cm wide, can later be obtained from a single graft. First, the skin is incised superficially and then the epidermis is removed from it by sharp dissection (deepithelialization) while maintaining constant tension. Fine petechial bleeding occurring in the dermis is a sign of proper dissection depth. Then the dermis is completely divided and the fatty tissue deep to it is mobilized down to a depth of 25 mm without injuring the muscle fascia. Then the tissue is removed en bloc, the donor site is closed, and the patient is positioned supine.
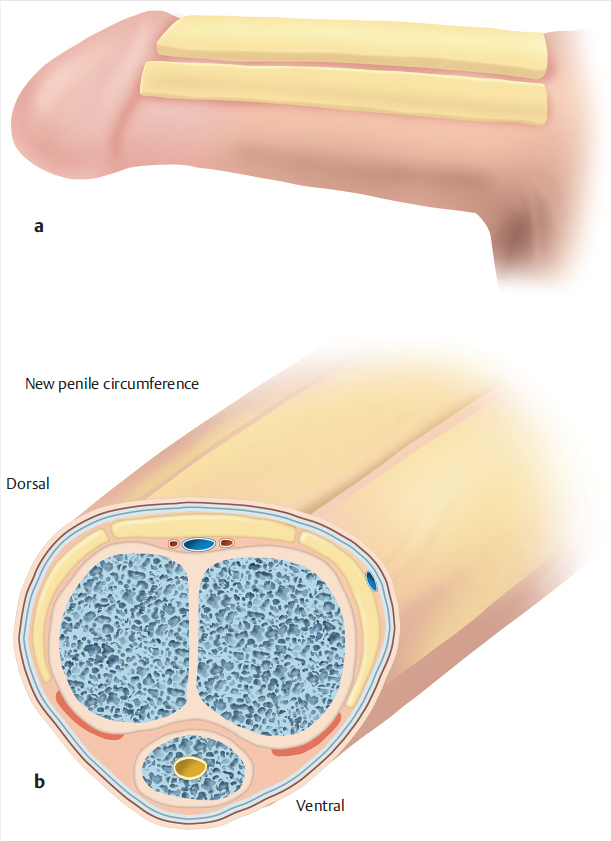
The graft is now adapted to the specific requirements. It is thinned accordingly, and its edges are beveled slightly so it will fit more easily into the recipient site. Then the graft is divided into three equal strips. A circular incision is made about 1 cm proximal to the corona of the glans. Then the tunica albuginea is exposed by dissecting the skin and the deep fascia of the penis (Buck’s fascia). The grafts are then each arranged dorsally and laterally and are anchored to the tunica albuginea with two to three simple interrupted sutures (e.g., with 2–0 Vicryl). The graft is then sized and placed under tension so that it fits distally into the coronary groove and ends proximally in the infrapubic region not far from the suspensory ligament of the penis. Then the Buck’s fascia and skin are drawn forward, and the edges of the wound are approximated and sutured in layers (▶Fig. 5.4a, b, ▶Fig. 5.5a, b).

Aftercare
Where present, the foreskin is fixed to the body of the penis with a strip of hypoallergenic tape to prevent movement or strangulation due to edema. The body of the penis is then wrapped in compresses, and the compresses are fixed. Then a bandage under tension toward the thigh is applied with another piece of adhesive tape to prevent strangulation of the penis. This tension is maintained for 7 to 10 days as otherwise the adipocutaneous grafts would be compressed, leading to adhesions that could later impair erectile function.
Complications
Irregularities in the surface or in the circumference of the body remaining after the healing phase can be managed by revision surgery or lipofilling (see Chapter 2.1.3, Fillers and Lipofilling in Genital Surgery), depending on their size. Necrosis of the skin of the penis is rare because of the good perfusion of the tissue. However, in some cases necrosectomy is necessary (▶Fig. 5.5c). In such cases, the resulting skin defect can usually be easily closed because of the good mobility of the surrounding skin. This means that using a split-thickness skin graft to cover a defect will only rarely be necessary.
5.2.3 Glans Augmentation
Surgical Procedure
The size of the glans varies greatly and can become more apparent after phalloplasty. Augmentations with hyaluronic acid or other preparations are relatively easy to perform. However, they usually have only a temporary effect. In contrast, surgical augmentations produce a permanent effect, yet because of the compact size of the glans they are relatively elaborate.
The most common indication for glans augmentation is status post penis augmentation, and for this reason glans augmentation should be included in the planning of a phalloplasty as a matter of course.
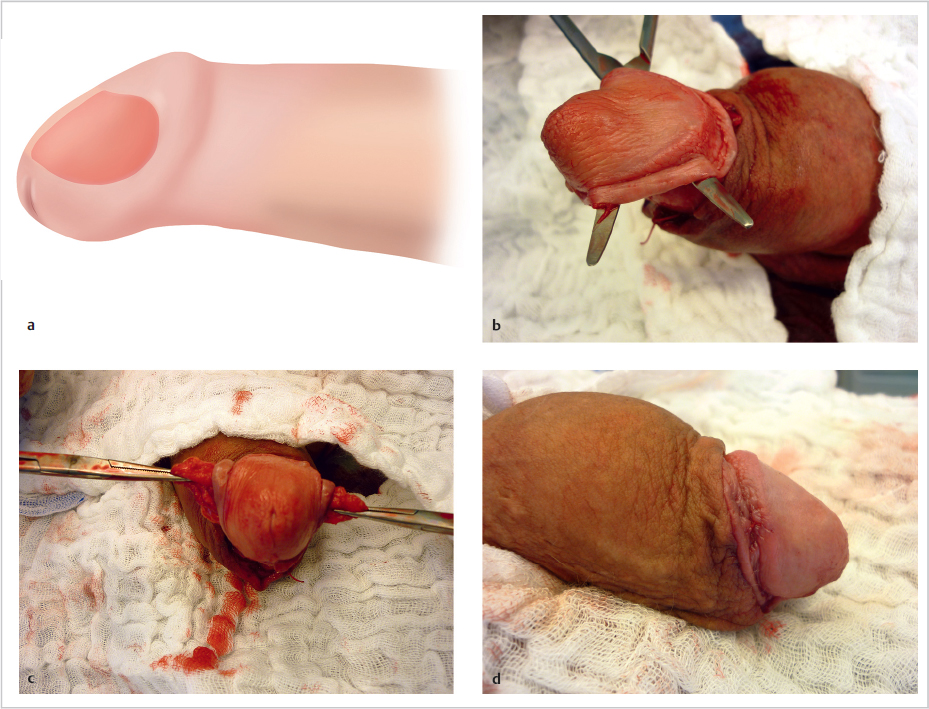
The principle of glans augmentation is the same as that of penis augmentation. An appropriately large adipocutaneous graft is harvested from the gluteal fold and processed accordingly (▶Fig. 5.6). Alternatively, it can be taken from the suprapubic region if repositioning the patient intraoperatively should be avoided.

Again, a circular incision is made about 1 cm proximal to the corona of the glans. Then the tunica albuginea is exposed by dissecting the skin and the deep fascia of the penis (Buck’s fascia).
The skin is undermined with blunt-tipped scissors distally as far as the margin of the corona. The dissected mantle of skin is then folded on the glans and slightly elongated, and the dissection is continued in the cleft between the glans and the corpora cavernosa. It is important to spare the navicular fossa of the urethra just proximal to the urethral meatus. Then a graft of the appropriate size is placed in the dissected cleft and sutured (▶Fig. 5.7a–d).
The wound is closed in layers, i.e., by approximating the wound edges of the cleft between the glans and corpora cavernosa, the Buck’s fascia (4–0 Vicryl), and the skin (4–0 Vicryl Rapide). Acellular dermal matrices are increasingly being discussed as an alternative to an adipocutaneous graft, and therefore this option must be discussed with affected patients (▶Fig. 5.8a, b).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


