4 Anesthesia and Safety Considerations in the Perioperative Period
Abstract
The massive weight loss patient demonstrates unique anatomic and physiologic characteristics that demand special attention to optimize anesthetic and perioperative safety. A team approach in the care of these patients, involving the surgeon, anesthesiologist, primary physician, nursing staff, and entire operating room staff, is extremely important. Preoperative work-up of these patients must include a thorough history and physical examination, as well as nutritional evaluation. These patients are at higher risk for anesthesia-related complications due to airway considerations, abnormal respiratory drive, increased risk of thromboembolism, and comorbid cardiac disease. Appropriate antibiotic and anti-thromboembolic prophylaxis must be employed, as well as careful patient positioning and body temperature control.
Introduction
The Institute of Medicine issued its report titled “To Err Is Human” in November 1999 and in it declared that the number of preventable deaths per annum in hospitals in the United States varied between 44,000 and 98,000.1,2 This startling revelation was based on data mined during inpatient chart reviews, and these numbers did not take into account outpatient procedures and their resulting complications. Thus, the actual number of deaths from preventable medical errors is most likely even higher. Safety in the perioperative period is a multifaceted concept whose implementation represents the capstone of the effort to improve the quality of care across all surgical disciplines. The issue of safety in the population of patients who elect to undergo body-contouring operations after massive weight loss is becoming a growing concern of particular interest to bariatric surgeons and plastic and reconstructive surgeons.
For nearly 25 years, obesity in the American populace has been on the rise, with the most current prevalence rates reported by the Centers for Disease Control and Prevention estimating that 34% of Americans age 25 or older are obese.3 The frequency with which the several bariatric procedures available are being performed has been on the rise, bolstered by evidence that these procedures improve and often resolve comorbidities such as hypertension and diabetes mellitus.4–6 Despite the recent economic recession, with lost wages and benefits, and an unemployment rate of nearly 10%, the popularity of postbariatric body-contouring operations persists.7 In fact, the number of bariatric operations skyrocketed in the last decade, going from only 13,000 in 1998 to nearly 200,000 in 2006.8 The American Society of Plastic Surgeons’ Body Contouring After Massive Weight Loss data show that the number of body-contouring operations performed by its members also had been on the rise from 2000 to 2007, and these figures actually only decreased by 12% from 66,947 in 2007 to 58,669 in 2008.9 With these large numbers of procedures being performed each year, it is incumbent on the medical field to ensure the prevention of medical errors and improve patient safety. When humans are involved, errors are inevitable. And despite technologic advances being made daily, errors continue to occur. The simple answer is that technology cannot prevent all human error.
What factors, then, should we rely upon to reduce medical errors, and what should be our goal Would we accept 90% or even 95% as the standard What about approximately 99.9% reliability—would that be good enough Take the highest of these—99.9% reliability—and consider if 1/10 of 1% away from perfect is acceptable. When we discuss medical errors, we often ask for the denominator, implying that there has to be some rate of preventable error that is acceptable in the practice of medicine. Most people would agree that 99.9% reliability is a great goal. But what, in fact, does 99.9% reliability mean when applied to other industries For example, if 99.9% reliability were allowable at Chicago’s O’Hare International Airport, where 2660 landings occur per day, then three crashes per day at that airport would be acceptable. Or apply the standard of 99.9% reliability to the United States Postal Service. Should we accept the loss of 7300 letters of the 7,300,000 letters delivered everyday Or would it be acceptable if 23,600 of the 23,600,000 iPods sold by Apple each year are defective It certainly would not be acceptable for the 99.9% reliability standard to be applied to Vanderbilt University Medical Center during the administration of medications, where over 14,000 doses are given each day, which would mean 14 patients per day were given the wrong dose. As these examples show, 99.9% accuracy would put most enterprises out of business.
So how do we accomplish greater than 99.9% accuracy Could we take a page from aviation for the answer Both the medical field and the airline industry have distinct but common facets that support the argument that management strategies for each could be used to achieve greater than 99.9% accuracy. For example, both fields are
Training and education intensive
Teamwork dependent
Time-constrained
Closely scrutinized
Highly stressful
Charged a high price for errors
Complex in their processes
Airlines achieve the goal of greater than 99.9% accuracy every day. Other industries could possibly achieve such results with similar implementation of processes for error management. In aviation, Crew Resource Management (CRM) has long been the strategy used to reduce the possibility of errors in flight. CRM is a paradigm initially adopted by the aviation community to help reduce the number of critical incidents in multipilot crew operations. It was designed to facilitate the improved communication among cockpit crew members during airline operations. Accident reports and cockpit voice recorder transcripts documented numerous incidents in which crew members hesitated to point out warning signs to the captain for fear of retaliation or punishment.
The initial incident that triggered this new approach was the 1978 crash of United Airlines flight 178 in Portland, Oregon. This event occurred because the captain was preoccupied with a landing gear malfunction and failed to monitor fuel level. The aircraft ran out of fuel and crashed on initial approach after the first officer and flight engineer had both warned the captain of the aircraft’s fuel status.10
CRM training emphasizes openness in communication of observations that may affect safety from any team member. The Agency for Healthcare Research and Quality (AHRQ) has adopted the CRM model as an “approach worthy of study.”11
This approach has been adopted in the very similar environment of the operating room by numerous hospitals. One author describes a “near-consensus” that CRM can improve safety.12 As applied in the surgical setting, it includes both preoperative briefings and postoperative review of any potential problems, as well as strong incentives for any team member to point out discrepancies in patient care.
CRM ensures that each team member is a resource and is based on the principle that the best decisions are made when information is systematically gathered, processed, and then acted upon. There are four key elements to CRM:
Teamwork and coordination
Recognition of adverse events
Communication between team members
Decision making
Thus, there are lessons that can be learned from the airline industry. Quite possibly we could improve the care of our patients with the routine application of these steps to our surgical practice. Interestingly, there is recent literature to support the idea that good teamwork alone among health care providers in the perioperative setting results in fewer adverse events and reduced mortality.13 In some ways, the principles set forth in CRM have already been applied for us, as exemplified by the Internet-Based Quality Assurance and Peer Review reporting system (IBQAP). Designed in 1999 by the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF), the IBQAP mandates biannual reporting of unanticipated sequelae, as well as random reviews of cases performed by all surgeons operating in AAAASF-accredited facilities. A review of over one million of these cases collected by the IBQAP was performed by Keyes et al,14 which revealed that the outpatient procedure most commonly associated with postoperative mortality from pulmonary embolism was abdominoplasty. In fact, abdominoplasty accounted for 13 of 23 deaths due to pulmonary embolism—more than 50%—and represents data that had been unknown prior to the implementation of the IBQAP initiative. This data acquisition and reporting system provides important information for perioperative patient safety by implementing the key strategies of CRM: coordinated teamwork among participating surgeons, recognition of adverse events in AAAASF facilities, and communication of these results in a way that facilitates improved decision making among plastic surgeons. The IBQAP represents but one step toward the goal of improved patient safety in plastic surgery, one step among many others that provide the basis for perioperative safety.
Measures for perioperative Safety in Massive Weight Loss Patients Undergoing Body-Contouring Surgery
Thorough Review of History and Physical
Safety considerations for massive weight loss patients who wish to undergo excisional body-contouring operations should begin with a thorough history and physical examination. Particular attention should be paid to the mechanism by which the patient has lost weight, whether by diet and exercise, pharmacotherapy, or a bariatric operation, as well as to the amount of weight that has been lost and the stability of the patient’s weight over the last 3 to 6 months post–weight loss. The import of the mechanism lies in the huge recurrence rate of weight gain in patients who have lost weight by diet and exercise, with evidence showing relapse rates that can exceed 90%.15,16 Further, pharmacotherapies can predispose massive weight loss patients to pathophysiologic changes as a result of the drugs themselves, as in the case of the now banned fenfluramine-phentermine, which is associated with a risk of valvular heart disease.17 Even alternative medications and supplements can predispose risk to patients in the perioperative period, such as ginseng tea, an energy-boosting supplement that has been associated with increased bleeding risk, and ma-huang, a cardiovascular stimulant used in dietary supplements that has been linked to stroke, myocardial infarction, and sudden death.18,19 And many patients who have achieved massive weight loss by bariatric operative means have, based on criteria for bariatric operations, comorbidities such as coronary artery disease, hypertension, and diabetes mellitus, among others, which can place them at risk in the perioperative setting for body-contouring operations.20 Obvious consideration should be placed on the patient’s allergies, surgical history, social history, and current medication list. Particular emphasis should be placed on the patient’s history of smoking, with its risks for infection, wound-healing problems, and venous thromboembolic disorders. In fact, some surgeons consider the vasoconstrictive effect of nicotine such a risk that they deem it a relative or even absolute contraindication for body-contouring surgery.21 The patient’s history of or current use of antiinflammatories and steroids, with their respective risks for bleeding and wound-healing problems, should be noted as well. A thorough assessment of these details allows for timely and appropriate preoperative clearance by our colleagues in medicine, cardiology, and anesthesiology, to allow for improved outcomes for body contouring.
Evaluation of Nutritional Status
As an extension of the evaluation of the patient’s medical history and general health status, preoperative nutritional status should be assessed as well, investigating macro- and micronutritive status. Standard preoperative laboratories, such as complete blood count with differential, electrolytes, albumin, and prothrombin time/international normalized ratio (PT/INR) and activated partial thromboplastin time (aPTT), may shed some light on some of these deficiencies, whose presence is not uncommon in massive weight loss patients, especially after malabsorptive bariatric procedures. Sebastian22 notes, however, that there are other derangements that can affect those seen in the standard work-up and can result from deficiencies of the following:
Folate—deficiency manifests as thrombocytopenia
Protein—deficiency manifests as protein calorie malnutrition, cachexia, and poor wound healing
Calcium—deficiency results in increased anesthetic risk and osteoporosis
Iron—deficiency manifests as microcytic anemia and fatigue
Zinc—deficiency results in poor wound healing and hair loss
Thiamin (vitamin B1)—deficiency results in Wernicke polyneuropathy
Vitamin B12—deficiency results in megaloblastic anemia, weakness, depression, and peripheral neuropathy
Vitamin A—deficiency results in night blindness and dry skin
Vitamin D—deficiency results in osteomalacia
In addition, the optimal serum albumin should be >3.5 g/dL, and any patients with preoperative hypoalbuminemia should be followed with serial prealbumin levels to assess improvement of anabolism with regard to protein stores.23,24 As a result of the possibility of these nutritive derangements and their potential for adverse outcomes after body contouring, massive weight loss patients should be optimized preoperatively to enhance their perioperative safety and improve surgical outcomes.
Beyond reviewing the preoperative risk assessment of the massive weight loss patient, there are other measures in perioperative safety that must be addressed to improve outcomes in body contouring. The routine use of perioperative antibiotics and their appropriate repeat dosing intraoperatively have had a profound effect on reducing surgical-site infections. Evaluation by an anesthesiologist preoperatively and intraoperative anesthesia care is essential to ensuring the best outcomes for the surgical patient, with particular attention being paid to maintaining normothermia, euvolemia, and hemodynamic stability. Other considerations, such as positioning, patient warming, and venous thromboembolism prophylaxis, are key elements in ensuring safe and effective care of the massive weight loss patient in the perioperative environment after excisional body-contouring surgery. But one of the most important contributions to improved perioperative safety is the routine use of a comprehensive “time-out.”
Handoff and Time-out Protocols
The most important aspects of communication (as adopted by the Joint Commission on the Accreditation of Healthcare Organizations) are the following:
Structured communication on handoffs
Read-backs on verbal orders
Identification of patient from two sources
Verification of correct patient, correct site, and correct procedure25
The concept of structured communication is an important one in helping to standardize communication of essential patient information during “handoffs” between one provider and another. This occurs both preprocedure, when the preoperative nursing team coordinates the transfer of care to the anesthesia and surgical teams, and postoperatively, when care is transferred either to the postanesthesia care unit (PACU) or intensive care unit (ICU) team. The essential information needed for safe transfer of care (perhaps between an anesthesia provider and a recovery room nurse) can be condensed into the mnemonic “SBAR.” Developed by the Kaiser Permanente system, the SBAR is a report composed of the broad categories of situation, background, assessment, and recommendations. This approach has been adopted by many institutions as a standard for transfer of patient care both within and outside of the perioperative environment. Clear communication during handoffs of responsibility can help to avoid both medication and procedural errors in care.
The other essential mechanism for patient safety in the perioperative setting is the advent and routine use of the preoperative time-out. According to the World Health Organization (WHO), after implementation of its Guidelines for Safe Surgery in 2008, the number of surgery-related deaths and mortality was reduced by one third.26
The WHO Surgical Safety Checklist has three phases: the “sign in,” which occurs before induction of anesthesia; the “time-out,” which occurs before skin incision; and the “sign out,” which occurs before the patient leaves the procedure or operating room ( Fig. 4.1 ).
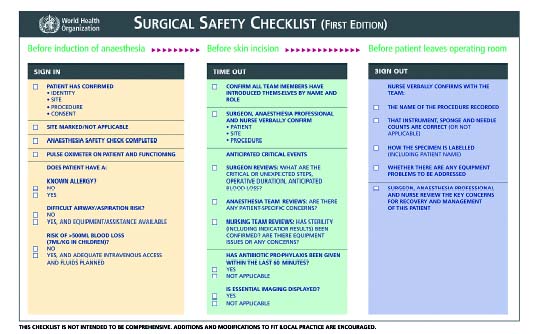
In the first phase, the sign in, the patient is awake and actively participating with members of the surgical team to confirm his or her own identity, that the surgical site and the proposed procedure are correct, and that informed consent has been obtained. The surgical site is then marked, and a pulse oximeter is placed on the patient and confirmed to be functional. An anesthesia checklist is also completed, with the assessment of patient allergies, airway/aspiration risk, and the potential for significant blood loss that may require additional intravenous access.
The second phase, the time-out, is performed prior to the surgical incision. At this time, all team members are to introduce themselves by name and role. This is then followed by the surgeon, anesthesia provider, and nurse verbally confirming the patient name, surgical site, and procedure. Anticipated critical events are then detailed, first by the surgeon, with regard to critical surgical steps, operative time, and anticipated blood loss. Next, the anesthesia provider verbalizes any patient-specific concerns, followed by the nurse confirming that there are no sterility, instrument, or other nursing-specific concerns. The presence or need for essential imaging is then confirmed. Finally, the administration of prophylactic antibiotics within 1 hour prior to incision is confirmed, or, in the case that it is not applicable, that scenario is confirmed as well.27 A recent study by Lingard et al28 found that 34% of pre-operative briefings demonstrated utility regarding improved patient care and interpersonnel communication, including identification of problems, resolution of critical knowledge gaps, decision making, and follow-up actions. They concluded that interprofessional checklist briefings reduced the number of communication failures and promoted proactive and collaborative team communication.
The third and final phase, the sign out, is performed before the patient is taken from the procedure or operating room. The nurse confirms with the surgical team the name of the procedure recorded; that instrument, sponge, and needle counts are correct; the name and labeling or any operative specimens; and whether there exist any equipment problems that require addressing. The checklist is then completed upon review of key concerns for the postoperative care of the patient by the surgeon, the anesthesia provider, and the surgical nurse.
The WHO Surgical Safety Checklist was recently implemented in a multinational study to assess its effect of on morbidity and mortality in a global population. In their article in the New England Journal of Medicine, Haynes et al29 found that the rate of inpatient complications was reduced from 11% to 7%, and that the mortality rate declined from 1.5% to 0.8%, with the use of the Surgical Safety Checklist.29
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2009 National Patient Safety Goals (NPSG) program sets forth a similar universal protocol for perioperative safety in several different settings, such as office-based surgery, ambulatory surgery, and hospital-based surgery.30 A multidisciplinary panel of widely recognized patient safety experts governs the development and annual updating of these patient safety goals, receiving additional input from other health care professionals who have hands-on experience in addressing patient safety issues in various health care settings.
Like the WHO Surgical Safety Checklist, the JCAHO NPSG program has a three-phase approach to improving perioperative safety: a preprocedure verification process, marking the surgical site, and performance of a time-out.31 The pre-performance verification process includes identifying the correct person, surgical site, and procedure at each of the following times:
At the time the procedure is scheduled
At the time of preadmission testing and assessment
At the time of admission or entry into the facility for a procedure, whether elective or emergent
Before the patient leaves the preprocedure area or enters the procedure room
Any time the responsibility for care of the patient is transferred to another member of the procedural team (including anesthesia personnel)
With the patient awake and aware when possible
Also, like the WHO checklist, the JCAHO NPSG protocol has a checklist that is used during the preprocedure verification process. This checklist requires that, in the preprocedure area, the relevant documentation (e.g., history and physical examination, nursing assessments, and anesthesia preoperative assessments), signed consents, diagnostic test results and radiographic materials, and any required blood products, implants, devices, or other special equipment be accurately matched to the patient. The second phase of the JCAHO NPSG protocol is also similar to the WHO checklist in that it involves marking of the surgical site, which is later visually and verbally confirmed during a time-out phase in each. The final phase of the JCAHO NPSG protocol is the time-out, which is the second portion of the WHO checklist. JCAHO recommends that its time-out be performed before induction of anesthesia and again before starting the procedure, as well as be standardized with characteristics defined by the hospital in which it is implemented. These characteristics include the following: the time-out is performed by a designated member of the health care team; verbal communication is used between members of the team so that concerns may be expressed; and a process exists for reconciling differences, should they exist. The components of the time-out as recommended by the JCAHO NPSG protocol are as follows: the correct patient identity is verified, the correct surgical site is marked, the patient is positioned appropriately, an accurate consent form is signed, there is agreement on the procedure to be performed, relevant images are displayed, the need for antibiotics or fluids intraoperatively is determined, and any special safety precautions that should be used given the patient’s history or medication use are determined.31 Though the WHO Surgical Safety Checklist and the JCAHO NPSG protocol are very similar in content, they are organized differently. Yet both provide a mechanism for coordinated efforts of health care providers to improve communication and thereby decrease adverse events.
Related posts:
 5 Propofol/Ketamine Anesthesia
5 Propofol/Ketamine Anesthesia
 7 The Anatomy and Chronology of Body Sculpting: Areas Requiring Correction and Timing of Procedures
7 The Anatomy and Chronology of Body Sculpting: Areas Requiring Correction and Timing of Procedures
 6 Factors Impacting Thromboembolism after Bariatric Body-Contouring Surgery
6 Factors Impacting Thromboembolism after Bariatric Body-Contouring Surgery
 8 Total Body Lift Surgery
8 Total Body Lift Surgery
 9 Postoperative Pain Management Following Body Contouring
9 Postoperative Pain Management Following Body Contouring
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


